Chemotherapy for Recurrent or Refractory Advanced Non-Small Cell Lung Cancer
Chemotherapy for Recurrent or Refractory Advanced Non-Small Cell Lung Cancer
Peter M. Ellis
Frances A. Shepherd
Publication of the Non-Small Cell Lung Cancer (NSCLC) Collaborative Group metaanalysis in 1995 established that first-line platinum-based chemotherapy is associated with a modest improvement in survival for patients with metastatic disease. 1 In general, most patients experience disease progression within a short time, with a median time to progression of approximately 4 months.2,3,4 However, at the time of progression, many patients maintain a good performance status (PS) and may be candidates for further systemic therapy. Even as recently as 1997 though, guidelines for the management of NSCLC stated, “there is no current evidence that either confirms or refutes that second-line chemotherapy improves survival in patients with advanced NSCLC.”5
Fortunately, substantial progress has been made over the last decade, and currently, numerous systemic therapeutic options are available for the treatment of advanced and metastatic NSCLC (Table 46.1). Several chemotherapeutic agents have been evaluated in the second-line setting. More recently, molecularly targeted agents have also shown benefit in this group of patients. Agents targeting the epidermal growth factor receptor (EGFR) and vascular endothelial growth factor (VEGF) have been widely investigated. As a result, multiple options now exist for second and subsequent lines of therapy for these patients.
This chapter will examine the available evidence for second-line treatment options for patients with NSCLC, progressing after first-line chemotherapy. Recommendations are based on data from randomized trials examining second-line treatment options for NSCLC. Published data were identified from a literature search using MEDLINE, as well as review of conference proceedings from meetings of the American Society of Clinical Oncology (ASCO), the International Association for the Study of Lung Cancer (IASLC), European Society of Medical Oncology (ESMO), and European Conference on Clinical Oncology (ECCO).
DOES SECOND-LINE CHEMOTHERAPY IMPROVE SURVIVAL AND/OR QUALITY OF LIFE?
Studies of second-line therapy in NSCLC are summarized in Table 46.2. The TAX 317 trial represents a milestone in the recent approach to second-line therapy for NSCLC. 6 This was a randomized trial of docetaxel versus best supportive care (BSC) for patients who previously had been treated with a platinum-containing (cisplatin or carboplatin) chemotherapy regimen. BSC could include treatment with antibiotics, analgesics, blood transfusions, and palliative radiation. Patients could have received more than one prior chemotherapy regimen, but were not eligible if they had received a prior taxane including paclitaxel. The study included patients with Eastern Cooperative Oncology Group (ECOG) PS 0 to 2. The primary outcome of TAX 317 was overall survival. Secondary outcomes included response rate, response duration, time to disease progression, and quality of life (QOL) (measured by the Lung Cancer Symptom Scale in North America and European Organization for Research and Treatment of Cancer quality of life questionnaire in Europe). In patients with measurable disease, response was assessed using bidimensional response criteria.
The planned dose of docetaxel was initially 100 mg/m2. However, an interim safety analysis by the Data Safety and Monitoring Committee identified five toxic deaths among 49 patients randomized to docetaxel 100 mg/m2 (D100). As a result, the protocol was amended and the dose of docetaxel was reduced to 75 mg/m2 (D75) in the second half of the study. The two dose levels of docetaxel were analyzed together in the primary analysis. Patients randomized to docetaxel could continue to receive chemotherapy until disease progression was documented, or there was unacceptable toxicity.
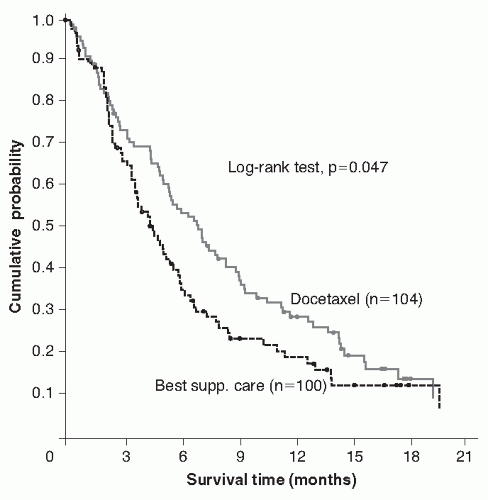
There were 204 patients randomized on the trial (BSC = 100; D100 = 49; D75 = 55). Baseline characteristics were generally well balanced between the groups. The TAX 317 trial demonstrated that docetaxel significantly improved survival compared to BSC, in patients who had received prior platinum containing chemotherapy (p = 0.047). The median and 1-year survival for patients randomized to docetaxel were 7 months (95% confidence interval [CI], 5.5 to 9.0) and 29%, respectively, compared with 4.6 months (95% CI, 3.7 to 6.0) and 19% for patients randomized to BSC (Fig. 46.1). The magnitude of this difference was slightly greater for patients randomized during the second phase of the trial to D75 or BSC (7.5 vs. 4.6; 1-year survival = 37% vs. 12%, p = 0.01).
TABLE 46.1 Major Advances in Second-Line Treatment of NSCLC over the Past Decade and a Half
* May not total 100% as the trial allowed patients with non-measurable disease.
BSC, best supportive care; CT, chemotherapy; Doc, docetaxel; Ifos, ifosphamide; NA, not applicable; NR, not recorded; OR, objective response; PD, progressive disease; Pem, pemetrexed; PS, performance status; SD, stable disease; TTP, time to progression; Vin, vinorelbine.
Hematological toxicities occurred commonly in patients receiving docetaxel. Grade 3 or 4 neutropenia was seen in 76% of patients, with febrile neutropenia occurring in 11.5% of patients overall, but only 1.8% of patients in the 75-mg/m2 group. Nearly 11% of patients had grade 3 or 4 anemia, but interestingly, a similar rate was observed among BSC patients. The predominant nonhematological toxicities occurring in the docetaxel group included asthenia, fever, infection, diarrhea, fluid retention, nausea, stomatitis, and neurologic. However, asthenia and infection were common adverse effects in the BSC group as well.
Supportive evidence that docetaxel is an effective second-line therapy for patients with NSCLC comes from the TAX 320 trial reported by Fossella et al.7 In this trial, patients were randomized to receive D100, D75, or a control arm (vinorelbine/ifosfamide [V/I]) of either ifosfamide (2 gm/m2 days 1 to 3 every 21 days) or vinorelbine (30 mg/m2 day 1, 8, and 15 every 21 days). In the docetaxel 100-mg/m2 group, granulocyte colony-stimulating factor (G-CSF) was used in subsequent cycles to manage prolonged neutropenia, or febrile neutropenia. As in the Tax 317 trial, participants could have received one or more prior therapy and the trial included patients with PS 0 to 2. However, unlike the trial by Shepherd et al. 6 participants could have received prior paclitaxel. QOL was measured using the Lung Cancer Symptom Scale.
FIGURE 46.1 Overall survival of docetaxel versus best supportive care (BSC; Tax 317). (From Shepherd FA, Dancey J, Ramlau R, et al. Prospective randomized trial of docetaxel versus BSC in patients with non-small-cell lung cancer previously treated with platinum-based chemotherapy. J Clinic Oncol 2000;18[10]:2095-2103.)
A total of 373 patients were randomized (D75 = 125; D100 = 125, V/I = 123). Compared to TAX 317, the patients were more heavily pretreated. A greater number of patients had received two or more prior chemotherapy regimens and more patients had disease progression as the best response to their last therapy. Between 31% and 42% of patients had received prior paclitaxel. Patients in the D75 group received more cycles of chemotherapy than those in the D100 group (median number of cycles 10 vs. 6). Both docetaxel groups had a significantly higher response rate than the V/I group (D100 = 10.8%, p = 0.001; D75 = 6.7%, p = 0.036; V/I = 0.8%). The response rate for patients who received prior paclitaxel was similar to the response rate for all patients. The median time to progression was similar among the three groups. However, progression-free survival (PFS) at 26 weeks favored the docetaxel groups (D100 = 19%, p = 0.013; D75 = 17%, p = 0.031; V/I = 8%). There were no significant differences in overall survival (median survival D100 = 5.5 months; D75 = 5.7 months; V/I = 5.6 months). However, there was a significant improvement in 1-year survival rate for the D75 group (D100 = 21%; D75 = 32%, p = 0.025; V/I = 19%). The observed toxicity was similar to that seen in the TAX 317 trial.
QOL was assessed in both TAX 317 and TAX 320,8,9 with the results demonstrating improvements in symptom scales in patients randomized to docetaxel. Dancey et al.8 reported a significant improvement in pain scores favoring docetaxel over BSC. Trends were also noted in favor of docetaxel for overall LCSS score, fatigue, and appetite. Mean overall QOL scores declined less in the docetaxel group than the BSC group.
These two landmark studies established the survival and QOL benefit from second-line chemotherapy with docetaxel for patients with NSCLC. These data are reflected in the 2003 updated ASCO guidelines for the treatment of unresectable NSCLC, which now recommend the use of docetaxel as second-line therapy for patients with adequate PS who have progressed following platinum-based chemotherapy. 10 Increasingly though, the decision to implement treatment guidelines has incorporated economic arguments in addition to data on therapeutic efficacy. As such, Leighl et al.11 performed an economic evaluation of the TAX 317 trial to determine the cost-effectiveness of docetaxel versus BSC in the Canadian environment. Costs were determined from resource utilization for patients entered on the trial from one tertiary academic center. Given the short survival overall for this group of patients, discounting was not employed. Efficacy data were taken from the overall trial results. The incremental cost of docetaxel was $57,749 per life year gained. However, the cost-effectiveness of D75 was only $31,776 per life year gained. In comparison to other health interventions, this is within a range of expenditure generally considered reasonable.
WHAT ARE THE APPROPRIATE DOSE AND SCHEDULE OF ADMINISTRATION OF DOCETAXEL?
The trials by Shepherd et al.6 and Fossella et al.7 established D75 administered every 21 days as the standard of care for second-line therapy for NSCLC. Over recent years, various investigators have explored alternate schedules of docetaxel in an attempt to improve the therapeutic ratio (Table 46.3). Nonrandomized comparisons of D100 and D75 in the TAX 317 trial showed no difference in efficacy and significantly more toxicity.6 Quiox et al.12 evaluated this question in a randomized phase II trial. Patients were randomized to D75 (n = 94) or D100 (n = 89). The response rate (7.4% vs. 7.6%) was similar as was the rate of disease control (45.7% vs. 57%). There were no significant differences in time to progression (D75 = 1.5 months; 95% CI, 1.3 to 2.0 months vs. D100 = 2.1 months; 95% CI, 1.3 to 2.7 months), or overall survival (D75 = 4.7 months; 95% CI, 3.8 to 5.9 months vs. D100 = 6.7 months; 95% CI, 4.8 to 7.1 months). More grade 3 and 4 neutropenia (72.7% vs.44%) and asthenia (19.1% vs. 8.6%) were observed with the higher dose of docetaxel. However, there was no difference in the rate of febrile neutropenia (6.8% vs. 6.7%). The rates of other nonhematological toxicities were similar between the two groups. The authors conclude that D75 every 3 weeks is the preferred dose because of a more favorable toxicity profile.
TABLE 46.3 Trials Comparing Alternate Doses and Schedules of Docetaxel
Doc 33, Docetaxel 33.3 mg/m2 weekly for 6 weeks followed by 2-week rest; Doc 35, Docetaxel 35 mg/m2 days 1,8,15, every 28 days; Doc 36, Docetaxel 36 mg/m2 weekly for 6 weeks followed by 2-week rest; Doc 40, Docetaxel 40 mg/m2 days 1 and 8 every 21 days, or weekly for 6 weeks followed by 2-week rest; Doc 75, Docetaxel 75 mg/m2 day 1 every 21 days; NA, not applicable; NR, not recorded; OR, objective response; PD, progressive disease; SD, stable disease; TTP, time to progression.
Some variation exists in the dose of docetaxel. In Japan, the dose of docetaxel routinely used is 60 mg/m2 every 3 weeks. This is based on data from a phase I clinical trial in which the maximum tolerated dose of docetaxel was found to be 70 mg/m2 every 3 weeks.13 As a result several Japanese phase II trials evaluated docetaxel at a dose of 60 mg/m2.14,15,16 Response rates, survival, and toxicity all appear comparable to the observed efficacy of docetaxel at a dose of 75 mg/m2 every 3 weeks in western populations. It is postulated that pharmacogenomic differences may exist between Japanese and North American populations to account for this difference.17,18
Five trials have evaluated docetaxel given in a weekly schedule versus the standard three weekly schedule.19,20,21,22,23 Di Maio et al.24 recently published an individual patient metaanalysis of these trials.24 The five trials randomized 865 patients to three weekly docetaxel (n = 433), or a weekly schedule (n = 432). Doses of docetaxel, in the weekly schedule, ranged from 33.3 mg/m2 to 40 mg/m2 weekly, either for 6 weeks followed by a 2-week rest, or for 3 weeks followed by a 1-week rest. There was no difference in survival between the two schedules of docetaxel (hazard ratio [HR] = 1.09; 95% CI, 0.94 to 1.26). The median survival for patients treated with three weekly docetaxel was 27.4 weeks compared with 26.1 weeks for patients treated with a weekly schedule. One-and two-year survival rates were 24.8% versus 27% and 10.3% versus 6.8%, respectively. Response rates were similar between the two groups (8.1% vs. 6.7%; p = 0.43). Weekly docetaxel was associated with significantly less grade 3 and 4 neutropenia (18% vs. 5%) and febrile neutropenia (6% vs. <1%). The available data suggest, therefore, that both the three weekly and weekly schedules of docetaxel can be used as second-line therapy for NSCLC. The toxicity advantages of weekly docetaxel may be counterbalanced by the increased frequency of treatment visits and associated increased resource utilization.
ALTERNATIVE CHEMOTHERAPY OPTIONS TO DOCETAXEL
Pemetrexed is a multitargeted antifolate with a broad spectrum of activity. It inhibits thymidine synthase, which is important in pyrimidine synthesis, as well as dihydrofolate reductase and glycinamide ribonucleotide formyltransferase, which are important enzymes in purine synthesis. Phase II trials have demonstrated activity of pemetrexed in NSCLC.25,26 Based on the phase II activity of pemetrexed, Hanna et al.27 conducted a randomized phase III trial of second-line therapy in NSCLC comparing pemetrexed to docetaxel.
The JMEI trial randomized patients to a standard arm of D75 every 21 days, or pemetrexed 500 mg/m2 every 21 days.27 Patients on the pemetrexed arm all received vitamin supplementation with folic acid and vitamin B 12 based on data from a trial of pemetrexed in malignant pleural mesothelioma.28 Dexamethasone premedication was used in both arms of the trial. Patients were excluded if they had received more than one prior chemotherapy for advanced disease, had prior docetaxel or pemetrexed, weight loss ≥10% in preceding 6 weeks, significant peripheral neuropathy (≥ grade 3), were unable to interrupt nonsteroidal anti-inflammatory drugs, or had uncontrolled pleural effusions (not further defined). The last two criteria relate to concerns about pemetrexed clearance. The study was designed to show that overall survival of patients randomized to pemetrexed was noninferior to that of docetaxel.
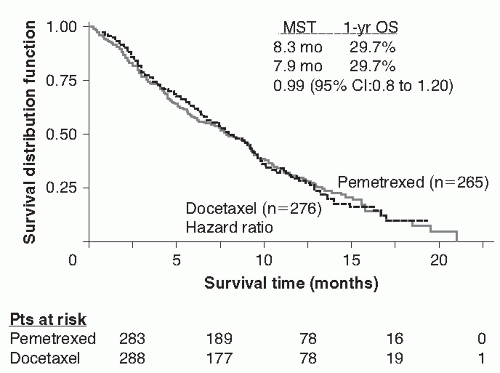
Five hundred and seventy-one patients were randomized (pemetrexed 283, docetaxel 288). The groups were well balanced regarding baseline characteristics. No differences were seen in any of the outcomes. The response rates (9.1% vs. 8.8%) and rates of disease stability (45.8% vs. 46.4%) were almost identical for pemetrexed and docetaxel, respectively. Prior paclitaxel therapy did not predict for any differential response. There were no differences in the PFS of pemetrexed compared with docetaxel (median PFS = 2.9 months vs.2.9 months; HR = 0.97; 95% CI, 0.82 to 1.16). Median survival (8.3 months vs. 7.9 months) and 1-year survival (29.7% vs.29.7%) of patients randomized to pemetrexed was not statistically different to that of docetaxel (HR = 0.99; 95% CI, 0.8 to 1.20; Fig. 46.2). The assumption of noninferiority was assessed using two methods. Using the percent retention method, the trial met its primary outcome of noninferiority. The alternate method of noninferiority defined pemetrexed as ≤10% worse than docetaxel. The trial did not meet this outcome of noninferiority as the upper limit of the 95% CI exceeded an HR of 1.11. Although this has created issues with some regulatory authorities, pemetrexed is generally considered to be an equally effective alternative to docetaxel as second-line therapy for NSCLC.
Although there were no differences in any of the efficacy parameters, there were some differences observed between the toxicities of pemetrexed compared with docetaxel. There was more hematological toxicity in patients receiving docetaxel compared with pemetrexed, and the rates of grade 3 and 4 neutropenia (40.2% vs. 5.3%) and febrile neutropenia (12.7% vs. 1.9%) were significantly higher in the docetaxel group. This resulted in a higher rate of hospitalization and G-CSF use. There were differences in nonhematological toxicities as well with more alopecia (37.7% vs. 6.4%), diarrhea (24.3% vs. 12.8%), and neurosensory toxicity (15.9% vs. 4.9%) among patients receiving docetaxel, but more nausea (16.7% vs. 30.9%), rash (6.2% vs. 14%), and liver enzyme abnormalities (1.4% vs. 7.9%) among patients receiving pemetrexed. Interestingly, despite these differences in toxicity, there were no differences in QOL between the two treatment groups.
FIGURE 46.2 Overall survival of docetaxel versus pemetrexed (JMEI). (From Hanna N, Shepherd FA, Fossella FV, et al. Randomized phase III trial of pemetrexed versus docetaxel in patients with nonsmall-cell lung cancer previously treated with chemotherapy. J Clin Oncol 2004;22[9]:1589-1597.)
A retrospective analysis of this trial was undertaken to explore predictors of survival for patients in the secondline setting.29 In univariate analyses, the following variables demonstrated associations with survival: sex (females = 9.4 months vs. males = 7.2 months, p = 0.001); stage at diagnosis (stage III = 9.5 months vs. stage IV = 7.8 months, p = 0.036); histology (adenocarcinoma = 9.1 months vs. squamous carcinoma = 6.5 months vs. other = 7.8 months, p = 0.004); PS (PS 0 = 12.7 months vs. PS 1 = 8.3 months vs. PS 2 = 2.6 months, p <0.001); best response to prior therapy (complete response [CR]/partial response [PR] = 15.8 months vs. stable disease [SD] = 10.5 months vs. progressive disease [PD] = 4.6 months, p <0.001); time from first-line to second-line therapy (≤3 months = 6.9 months vs. 3 to 6 months = 9.2 months vs. ≥6 months = 9.3 months, p = 0.001); and first-line regimen (platinum-gemcitabine = 9.1 months vs. platinum-taxane = 7.4 months vs. other = 7.8 months, p = 0.63). The authors conclude that these variables should be used as stratification variables in future randomized trials. However, given the retrospective nature of these analyses, these variables should not be used to select between docetaxel and pemetrexed.
A further retrospective analysis of the JMEI trial suggested that there may be a difference in the effectiveness of pemetrexed compared with docetaxel based on histology. 30 Previous research has suggested thymidine synthase expression may be higher in squamous carcinoma compared with other histological subtypes.31 This is postulated to reduce the sensitivity of squamous carcinoma to pemetrexed. Peterson et al.30 reported that survival of patients with squamous carcinoma treated with pemetrexed was less than that of patients treated with docetaxel (6.2 months vs. 7.4 months; HR = 1.563; 95% CI, 1.079 to 2.264). Interestingly, they also observed an improvement in survival for patients with nonsquamous histology treated with pemetrexed (9.3 months vs. 8.0 months; HR = 0.778; 95% CI, 0.607 to 0.997).
Only gold members can continue reading. Log In or Register to continue