Chemotherapy for Advanced Non-Small Cell Lung Cancer
Chemotherapy for Advanced Non-Small Cell Lung Cancer
Leora Horn
Cesare Gridelli
Corey Langer
David H. Johnson
Lung cancer is the leading cause of cancer-related mortality worldwide.1,2 In North America and Europe, an estimated 40% of all newly diagnosed non-small cell lung cancer (NSCLC) patients present with advanced-stage disease (stage IIIB with pleural effusion or stage IV). Moreover, a significant number of patients who present with early stage NSCLC will eventually relapse with extrathoracic metastases. When managed with supportive care alone, these patients experience a median survival of approximately 4 to 5 months and 1-year survival rates of around 10%.3,4 For more than 6 decades, clinical investigators have labored to improve on these results with little success.5,6 Early efforts were hampered by the use of relatively inactive cytotoxic agents.7 Subsequent attempts to improve outcome were predicated on the supposition that combination therapies could increase antitumor activity while minimizing host toxicity.8 However, with rare exception, the early clinical trials comparing combination chemotherapy to supportive care alone failed to yield a meaningful survival benefit. Although the negative outcome of these trials was commonly attributed to lack of efficacy of the available drugs, some experts posited the initial studies simply lacked adequate statistical power to detect a modest, but clinically important improvement in survival. To remedy this shortcoming, a metaanalysis of the extant data was undertaken in 1995.9 This landmark study confirmed the lack of a survival benefit with chemotherapy regimens comprised of alkylating drugs or vinca alkaloids; however, NSCLC patients treated with cisplatin-based therapy were shown to have a survival advantage over those given supportive care alone (hazard ratio [HR] = 0.73; p <0.0001). The survival advantage amounted to a 1.5-month increase in median survival and a 10% improvement in 1-year survival. Platinum-based chemotherapy was subsequently shown to be cost-effective and capable of improving quality of life.10,11
In a recent update of the 1995 metaanalysis, six randomized clinical trials (RCT) and an additional 1702 patients were added to the previously analyzed database.12 In total, the updated analysis included 15 randomized studies involving 2666 patients. Eleven of the trials employed cisplatin-based chemotherapy, whereas four studies involved a comparison of single agents (etoposide, vinorelbine, gemcitabine, or paclitaxel) and supportive care alone. The results of the updated metaanalysis affirmed the previously identified survival benefit of chemotherapy (HR = 0.78; 95% CI, 0.71 to 0.84; p <0.000001). Somewhat surprisingly, there was no apparent difference in the magnitude of effect between trials that used cisplatin-based regimens or the single agents. Moreover, there was also no evidence that any patient subgroup as defined by age, sex, stage, or histology benefited more or less from chemotherapy. The absolute survival benefit of chemotherapy at 1-year did vary according to World Health Organization (WHO)/Eastern Cooperative Oncology Group (ECOG) performance status (PS) 0 = 8% (from 26% to 34%), PS 1 = 8% (from 18% to 26%), PS 2 = 5% (from 6% to 11%), and PS 3 = 4% (from 5% to 9%). The updated metaanalysis suggests the effectiveness of newer agents such as vinorelbine, paclitaxel, and gemcitabine is similar to that of cisplatin combined with older agents such as vindesine or mitomycin (see succeeding discussion) and also reaffirms the substantial and consistent relative survival benefit of chemotherapy in advanced NSCLC.12
Although the improvement in the survival of patients with advanced NSCLC is caused, in part, by better chemotherapy, as outlined previously, changes in the natural history of NSCLC may have also played a role. Wakelee et al.13 analyzed all advanced NSCLC ECOG trials conducted between 1981 and 2000. These investigators first assessed changes in demographic factors and treatment regimens and then correlated these findings with survival outcome among patients diagnosed between 1981 and 1990 compared to those diagnosed from 1991 to 2000. Survival was clearly better, in the trials conducted between 1991 and 2000, explained in part by favorable changes in eligibility criteria (e.g., more women and more favorable patterns of metastases). However, these investigators also observed a change in the natural history of the disease. For example, there was a longer time to progression suggesting that improved chemotherapy yielded improved survival in the post-1990 era. They also observed a longer interval between disease progression and death, suggesting second-line therapies and supportive care options improved after 1990. Although these observations are conceivably caused by the enrollment of patients with more indolent disease after 1990 or the earlier detection of less symptomatic, advanced NSCLC, this seems less likely. Regardless, the results of this retrospective analysis are consistent with the hypothesis that the improved survival observed over the past decade in patients with advanced NSCLC is indeed multifactorial.
TABLE 45.1 Phase III Trials of Third-Generation Drugs and BSC in Advanced NSCLC
BSC, best supportive care, CT, chemotherapy; RR, response rate; MST, median survival time; NSCLC, non-small cell lung cancer.
THE EVOLUTION OF CHEMOTHERAPY IN ADVANCED NSCLC
In the latter part of the 20th century, a number of new cytotoxic agents, including vinorelbine, paclitaxel, docetaxel, gemcitabine, irinotecan, and pemetrexed, were found to possess single-agent activity in advanced NSCLC.14 Collectively, these agents are known as third-generation drugs to distinguish them from older agents such as etoposide, ifosfamide, mitomycin, and vindesine, which are often referred to as secondgeneration drugs. In some cases, single-agent administration of these third-generation drugs has yielded a modest survival benefit when compared to supportive care (Table 45.1).14,15,16 When a third-generation drug is combined with a platinum compound, objective response and survival rates are improved compared to the same third-generation drug used alone 17,18,19 and 20 (Table 45.2). Similarly, a third-generation drug combined with a platinum agent produces better responses and improved survival compared to single-agent cisplatin21,22 and 23 (Table 45.3). Under either circumstance, however, the higher response rates and improved survival come at a cost of increased host toxicity albeit with no increase in treatment-related mortality. 20 In general, and most importantly, third-generation platinum-based doublet chemotherapy regimens tend to produce higher response rates and superior overall survival (OS) compared to second-generation platinum-based doublet therapies 24-28 (Table 45.4). Interestingly, the survival improvement observed with some of the third-generation agents used alone is comparable to that achieved with platinum doublets employing second-generation drugs 29,30 (Table 45.4).
TABLE 45.2 Trials Comparing Third-Generation Doublets and Single Agents in NSCLC
Following the development of third-generation platinum-based regimens, randomized trials were undertaken to compare their respective activities31,32,33,34,35,36,37 (Table 45.5). Typical of these studies was a trial conducted by the ECOG (E1594) in which chemotherapy-naive patients with advanced NSCLC were randomized to receive cisplatin plus paclitaxel, considered a reference regimen based on an earlier ECOG trial, 26 or one of three regimens employing a third-generation drug: cisplatin plus gemcitabine, cisplatin plus docetaxel, or carboplatin plus paclitaxel.31 Overall response rates and survival did not differ significantly between the reference regimen of cisplatin and paclitaxel and the three investigational arms. Comparable outcomes have been reported by others.32,33,34,35,36,37 Although there were some modest differences in the responses rates and survival among these trials, they are almost certainly a result of subtle, although critical differences in the study population characteristics.13 For example, the survival rates in the TAX-326 study appear superior to other trials 35; however, approximately one third of the participants in TAX-326 had stage III disease, compared with just 13% of the patients enrolled in the ECOG study E1594.31 In some cases, the toxicity profiles appear to be quite different, especially among studies carried out exclusively in Asia.36 Most likely, the different toxicity profiles are caused by ethnic differences in drug metabolism.38 Regardless, no truly clinically relevant survival differences have emerged among the commonly used third-generation platinum-based doublet regimens. Taken together, these data indicate that third-generation platinum-based doublets represent the current standard of care in patients with advanced NSCLC and good PS (PS 0 to 1).4,14
TABLE 45.4 Trials Comparing Second-and Third-Generation Doublets in NSCLC
ECOG, Eastern Cooperative Oncology Group; EORTC, European Organisation for Research and Treatment of Cancer; FACS, Four-Arm Cooperative Study; H3H-MC-JMDB, H3H-MC-Japanese Medical Database; ILCP, Italian Lung Cancer Project; SWOG, Southwest Oncology Group; TAX-326, Taxotere-326 Trial.
Triplet versus Doublet Platinum-Based Drug Combinations A time-honored strategy for improving the effectiveness of cytotoxic therapy is to combine multiple agents with different mechanisms of action and nonoverlapping toxicities.39 Thus, adding a third active drug to the aforementioned third-generation platinum doublets has considerable theoretical appeal given their improved activity and favorable toxicity profiles.40,41 In fact, triple-drug combinations have demonstrated good tolerability and excellent activity in both phase II and phase III trials.29 However, in two separate metaanalyses of the extant data, improved overall response rates failed to result in an increase in OS40,42 (Table 45.6). In addition, host toxicity is greater with triple drug therapy.30,40 Together, these data indicate triplet drug chemotherapy is not appropriate for patients with advanced NSCLC outside the confines of a clinical trial.
Duration of Therapy The duration of initial chemotherapy administration in advanced NSCLC is a matter of some controversy.30 American Society of Clinical Oncology (ASCO) practice guidelines recommend no more than six cycles in responding patients, the American College of Chest Physicians guidelines recommend no more than three to four cycles, whereas the National Comprehensive Cancer Network (NCCN) guidelines are basically noncommittal on this topic.43,44,45 The lack of agreement among the various guidelines is perhaps not too surprising given the relative paucity of adequately powered prospective studies addressing this issue 46-49 (Table 45.7). Among the first to tackle this issue were Smith et al.46 who randomized advanced NSCLC patients to three versus six cycles of mitomycin, vinblastine, and cisplatin. Median (6 vs. 7 months) and 1-year survival rates (22% vs. 25%; p = 0.2) as well as the median durations of symptom relief (4.5 months in both arms) were essentially identical in the two arms. Quality-of-life parameters also were the same or improved for patients randomized to only three courses, including a significant decrease in fatigue (p = 0.03) and a trend toward decreased nausea and vomiting (p = 0.06). von Plessen et al.48 reported nearly identical results using carboplatin plus vinorelbine. Both studies employed relatively modest doses of platinum drug, which may have influenced the outcomes. However, there is little evidence for a cisplatin-dose response in NSCLC50,51 rendering this potential criticism somewhat mute. Moreover, in patients with stages IIIB or IV NSCLC, investigators at the University of North Carolina compared four cycles of standard doses of carboplatin and paclitaxel every 3 weeks to continuous treatment with these agents until disease progression.47 Fifty-seven percent of patients allocated to four cycles completed the intended course of chemotherapy. Patients randomized to the continuous treatment arm received a median of four cycles of chemotherapy; 42% received ≥5 cycles of carboplatin and paclitaxel. Overall response rates (22% vs. 24%; p = 0.80), median survival (6.6. vs. 8.5 months), and 1-year survival rates (28% vs. 34%; log rank p = 0.63) were comparable and not statistically different. Hematologic and nonhematologic toxicity rates also were similar between the two arms, whereas neuropathy was more common in the continuous treatment arm (14% vs. 27%; p = 0.02). There were no differences in quality-of-life parameters. The frequency of patients who received second-line therapy was identical in the two groups as well (42% vs. 47%; p = 0.42).
TABLE 45.6 Metaanalyses Addressing Number of Drugs in Advanced NSCLC
Adapted from Delbaldo C, Michiels S, Syz N, et al. Benefits of adding a drug to a single-agent or a 2-agent chemotherapy regimen in advanced non-small-cell lung cancer: a meta-analysis. JAMA 2004;292(4):470-484.
NA, not applicable; NSCLC, non-small cell lung cancer.
TABLE 45.7 Phase III Trials: Duration of Chemotherapy in Advanced NSCLC
The likely death knell for prolonged duration therapy came from a study conducted by the Korean Cancer Study Group.49 Patients with advanced NSCLC who had not progressed after two induction courses of a third-generation platinum-based chemotherapy were subsequently randomized to four or six additional cycles of chemotherapy. The study population presumably represents a subset of patients with the highest probability of benefiting from extended duration of therapy because they had already demonstrated “platinum sensitivity.” Nonetheless, there was no improvement in response rate (43% vs. 42%) or survival (15.9 vs. 14.9 months) with six additional cycles of chemotherapy although time to disease progression was improved. Moreover, patients randomly assigned to four cycles were more likely to receive second-line treatment, experienced less toxicity, and regained their functional status more rapidly than those patients randomly assigned to six cycles.
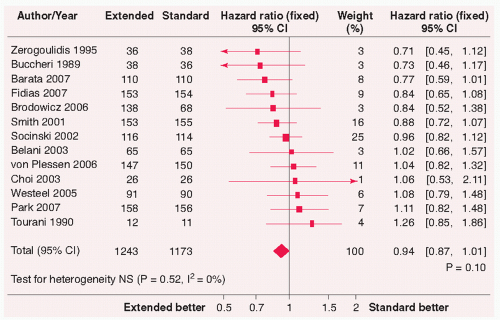
A recent metaanalysis including 13 trials and 2416 patients found a significant improvement in progression-free survival (PFS) (HR = 0.78; 95% CI, 0.72 to 0.86; p <0.0001) but no improvement in OS (HR = 0.94; 95% CI, 0.87 to 1.10; p = 0.1) as well as increased toxicity and decreased quality of life for longer duration chemotherapy 52 (Fig. 45.1). The improvement in PFS was greater for third-generation regimens (HR = 0.73 vs. 0.92; p = 0.02). Interestingly, when a trial of maintenance pemetrexed conducted by Ciuleanu et al.53 (see next discussion) was added to the analysis there was a significant, albeit modest improvement in OS (HR = 0.92, 95% CI, 0.86 to 0.99; p = 0.03).52 This trend is likely caused by the fact that the Ciuleanu study enrolled 663 patients, almost 3 times the number of all other studies included in the analysis, therefore, significantly influencing the study results. In addition, the addition of the Ciuleanu study to the metaanalysis is questionable as all other trials included in the analysis compared maintenance doublet chemotherapy to no further therapy, whereas the study by Ciuleanue et al. used maintenance single-agent therapy.
Collectively, these data indicate treatment beyond three to four cycles of platinum-based therapy is of limited to no benefit in patients with advanced NSCLC.30,54,55 Rather than employing prolonged administration of a first-line platinumbased therapy, a more patient-friendly strategy would appear to be the attentive use of sequential single active agents after initial induction therapy.56 Future research efforts should concentrate on diagnostic methodologies that would allow oncologists to select patients who are more likely to benefit from a particular therapy instead of continued efforts to optimize treatment duration with existing therapies.56
FIGURE 45.1 Overall survival for extended versus standard chemotherapy. 52 The summary HR 0.94 (95% CI, 0.87 to 1.01; p = 0.10) suggests no benefit to extended chemotherapy. It should be noted when an additional study by presented by Cuilenau et al. 53 at the same meeting was included in the analysis the HR marginally improved to 0.92 (95% CI, 0.86 to 0.99; p = 0.03). CI, confidence interval. (From Soon Y, Stockler MR, Boyer M, Askie L. Duration of chemotherapy for advanced non-small cell lung cancer: An updated systematic review and metaanalysis. ASCO Meeting Abstracts 2008;26[15 Suppl]:8013.)
Maintenance Therapy Two large randomized controlled trials have demonstrated improvements in PFS 57,58 and OS 57 when chemotherapy, paclitaxel and carboplatin 57 or gemcitabine and cisplatin 58 were combined with bevacizumab, a monoclonal antibody targeting vascular endothelial growth factor (VEGF) in patients with nonsquamous NSCLC. Based on these results, Patel et al.59 conducted a phase II trial of pemetrexed and carboplatin plus bevacizumab with maintenance pemetrexed and bevacizumab in patients with advanced nonsquamous NSCLC and found a response rate of 55% (95% CI, 51% to 69%) median PFS of 9.3 months and OS of 13.5 months (Table 45.8).
Ciuleanu et al.53 conducted a randomized phase III trial in patients who had responded to four cycles of platinum-based chemotherapy comparing maintenance single-agent pemetrexed to best supportive care. Early treatment with pemetrexed was associated with a significant improvement in PFS (4.04 vs. 1.79 months; p <0.00001) and trend toward improvement in OS (13.0 vs. 10.2 months; p = 0.060). Similar to prior studies evaluating pemetrexed in NSCLC, the benefit was limited to patients with nonsquamous cell histology NSCLC.37 It should be noted that in this trial, only 50% of patients receiving best supportive care received second-line chemotherapy of which only 11.2% received pemetrexed. It is not known how many patients in the best supportive care arm that received third-line chemotherapy, which was administered to 37% of pemetrexedtreated patients. Treatment with pemetrexed was associated with significantly more serious adverse events (4.3% vs. 0%) and grade 3 or 4 adverse events (14.3% vs. 3.6%; p <0.001).
Maintenance therapy with gefitinib after three cycles of chemotherapy was compared to continued platinum-doublet chemotherapy, up to six cycles of carboplatin plus paclitaxel, cisplatin plus irinotecan, cisplatin plus vinorelbine, cisplatin plus docetaxel, or cisplatin plus gemcitabine in Asian patients with advanced NSCLC.60 Chemotherapy was associated with a significantly higher incidence of anemia (22% vs. 13.3%), whereas rash and elevations in liver function tests occurred in 4% and 11% of gefitinib-treated patients, respectively. The median number of chemotherapy cycles was three in both treatment groups. There was a similar response rate between treatment groups. Patients treated with gefitinib had a significant, albeit, small improvement in PFS (4.6 vs. 4.3 months; p <0.001) but no difference in OS (13.7 vs. 12.9 months; p = 0.10). In a prespecified subset analysis of patients with adenocarcinoma, approximately 80% of study patients, treatment with maintenance gefitinib was associated with a significant improvement in OS (15.4 vs. 14.3 months; p = 0.03). Although not significant, patients with nonadenocarcinoma receiving maintenance gefitinib had a worse OS compared to chemotherapy alone (7.7 vs. 9.2 months; p = 0.24). When patients were stratified by smoking status, never-smokers appeared to have a better OS regardless of therapy compared to smokers. Smokers with adenocarcinoma appeared to have an improvement in OS with maintenance gefitinib compared to chemotherapy alone (13.6 vs. 10.0 months; p = 0.003). Interestingly, although not significant, never-smokers receiving maintenance gefitinib appeared to have a worse OS compared to chemotherapy alone (21.6 vs. 23.5 months; p = 0.72). Therefore, it appears that maintenance gefitinib following platinum-based chemotherapy may be beneficial in a subset of patients with adenocarcinoma. A large randomized phase III trial, comparing maintenance erlotinib to placebo following treatment with carboplatin and paclitaxel with or without bevacizumab (ATLAS), has closed to accrual in North America and results are expected to be reported in late 2009.
Chemotherapy regimens: carboplatin plus palitaxel, cisplatin plus irinotecan, cisplatin plus vinorelbine, cisplatin plus docetaxel, cisplatin plus gemcitabine.
CT, chemotherapy; MST, median survival time; NSCLC, non-small cell lung cancer; PFS, progression-free survival; RR, response rate; TTP, time to progression.
Cisplatin versus Carboplatin Whether to use cisplatin or carboplatin as the platinum agent of choice in frontline therapy is another of the more enduring controversies surrounding the treatment of advanced NSCLC.61,62 The controversy intensified with the publication of two prospective trials that demonstrated a superior survival in advanced NSCLC patients treated with cisplatin-based third-generation doublets as compared to carboplatin-based third-generation doublets 35,63 (Table 45.9).
Two recent metaanalyses have examined the clinical relevance of cisplatin versus carboplatin in frontline treatment for advanced NSCLC.61,62 The first of these was a literature-based analysis of eight trials that directly compared cisplatin-and carboplatin-based doublets, five of which employed a third-generation doublet.61 A total of 2948 patients were enrolled in these trials. Cisplatin-based chemotherapy produced a statistically significant higher response rate (OR = 1.36; 95% CI, 1.15 to 1.61; p <0.001) but no survival advantage (HR = 1.050; 95% CI, 0.907 to 1.216; p = 0.515). However, in the subgroup of trials that employed third-generation drugs, cisplatin-based combinations yielded a survival benefit compared to carboplatin-based doublets (HR = 1.106; 95% CI, 1.005 to 1.218; p = 0.039).
The second metaanalysis, the so-called CISCA (CISplatin vs. CArboplatin) study, 62 was based on individual patient data from nine randomized trials that involved a total of 2968 patients.31,35,63,64,65,66,67,68 The objective response rate was higher for patients treated with cisplatin than in the cohort treated with carboplatin (30% vs. 24%, respectively; OR = 1.37; 95% CI, 1.16 to 1.61; p <0.001). Notably, carboplatin treatment was associated with a nonstatistically significant increase in the hazard of mortality relative to treatment with cisplatin (HR = 1.07; 95% CI, 0.99 to 1.15; p = 0.100) (Fig. 45.2). Cisplatin-treated patients experienced a median survival and 1-year survival rate of 9.1 months and 37%, respectively, whereas carboplatin-treated patients had a median survival of 8.4 months and a 1-year survival rate of 34%. In patients with nonsquamous tumors and those treated with third-generation chemotherapy, carboplatin-based chemotherapy was associated with a statistically significant increase in mortality (HR = 1.12; 95% CI, 1.01 to 1.23 and HR = 1.11; 95% CI, 1.01 to 1.21, respectively). The authors opined that cisplatin-based third-generation regimens should remain the standard reference for the treatment of selected patients with advanced-stage NSCLC.62 Parenthetically, it may be worth noting that the subset of patients who seemingly derived the greatest benefit from cisplatin is the same subset of patients that appear to benefit from the addition of bevacizumab to frontline chemotherapy (see succeeding discussion).
TABLE 45.9 Cisplatin versus Carboplatin Chemotherapy in Advanced NSCLC