PATIENT HISTORY AND PHYSICAL FINDINGS
■ A thorough history should be obtained prior to intervention and should include a detailed description of, if present, symptoms (quality, duration, etc.) that may be indicative of transient ischemic attacks (TIA) or prior stroke, past medical/surgical history (e.g., prior cerebrovascular disease/interventions), current medications (e.g., antiplatelet or anticoagulation medications), and social history (e.g., tobacco use).
■ A comprehensive physical exam is mandatory and should include a complete vascular and neurologic/stroke evaluation. Vascular exam should note the presence of palpable femoral and distal lower extremity pulses and carotid bruits.
IMAGING AND OTHER DIAGNOSTIC STUDIES
■ Initial carotid duplex ultrasound is obtained to evaluate the degree of stenosis and plaque morphology. Studies have highlighted a higher potential for embolism during CAS with hypoechoic lipid-containing plaque.4
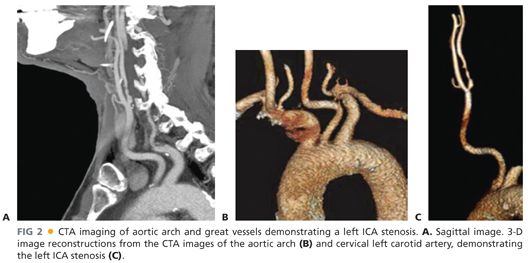
■ Angiographic imaging of the aortic arch and carotid and cerebral arterial vasculature must be obtained to aid in proper patient selection and procedural planning. This is accomplished through computed tomographic arteriography (CTA) (FIG 2), magnetic resonance arteriography (MRA), or catheter-based contrast arteriography.
■ Arch anatomy
■ Aortic arch morphology is variable and can change with advancing age. The arch anatomy can be divided into three types, dictated by the position of the innominate artery origin relative to two horizontal lines drawn across the apices of the outer and inner aortic arch curvatures (FIG 3).
■ Type I—the innominate origin arises at or above the horizontal plane of the outer arch curvature (FIG 3A)
■ Type II—the innominate origin arises in between the two horizontal planes of the outer and inner arch curvatures (FIG 3B)
■ Type III—the innominate origin lies below the horizontal plane of the inner arch curvature (FIG 3C)
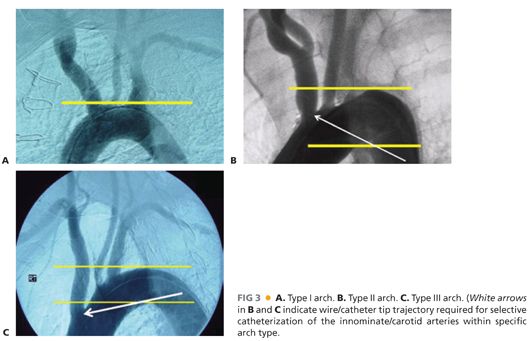
■ The difficulty in gaining access to the carotid arteries increases from types I to III. There is an increase in angle acuity of the great vessel origins off the arch with increasing arch types that make wire/catheter guidance/exchange more difficult.
■ Bovine arch—congenital arch variations where the left common carotid artery (CCA) shares a common origin with the innominate artery (more frequent) or the left CCA branches off the innominate artery. In a pure bovine arch (extremely rare), the right subclavian, common carotid—both right and left—and left subclavian all derive from one common arterial trunk off the aortic arch.
■ Shaggy aorta—when extensive aortic wall irregularities exist, there is a high risk for significant atheroembolism and thus, this may be a contraindication to CAS.
■ Eggshell aorta—with severe aortic wall calcification, there is increased risk of intimal disruption and difficulty of wire/catheter manipulation/advancement.
■ Cerebral flow to both hemispheres is assessed to determine cerebral reserve.
■ Carotid vessel size, tortuosity, and calcification—carotid artery diameter should be assessed to aid in determining device sizes. In addition, severe carotid circumferential calcification and vessel tortuosity may negatively impact procedural success (e.g., difficulty with inserting stent, placement of EPD in distal ICA) and may represent a contraindication to CAS.
■ Preoperative brain imaging with computed tomography (CT) or magnetic resonance imaging (MRI) is needed for symptomatic patients to document prior infarcts and to rule out preexisting hemorrhagic stroke prior to the initiation of the procedure.
SURGICAL MANAGEMENT
■ The indications for any surgical intervention for carotid disease depend on the patient’s clinical status (i.e., symptomatic or asymptomatic) and the characteristics of the carotid lesion.
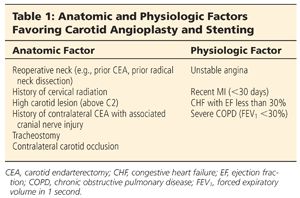
■ It has been widely accepted that appropriate candidates for CEA are symptomatic patients with carotid stenosis of 70% to 99% on noninvasive imaging and an anticipated perioperative risk of stroke or mortality of less than 6%. Benefit of intervention for symptomatic patients with lesser degrees of stenosis (50% to 69%) has also been shown but not for symptomatic patients with less than 50% carotid stenosis. CAS is an alternative to CEA for symptomatic patients meeting similar criteria along with anatomic and/or physiologic factors unfavorable for CEA (Table 1).3,5
■ The recommendations/indications for CAS in asymptomatic patients are still issues for debate and no consensus exists. CAS may be considered for patients with asymptomatic ICA stenosis between 70% and 99%, but there are insufficient data to recommend CAS for primary therapy in asymptomatic patients. Therefore, these patients need to be addressed on a case-by-case basis with consideration of patient comorbidities and risks of CAS.
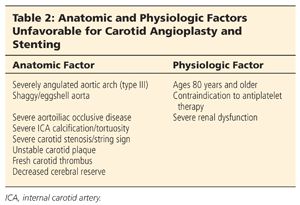
■ The contraindications for CAS are predominantly related to aortic arch and carotid artery anatomic factors (Table 2).
Preoperative Planning
■ Patients are initiated on antiplatelet therapy with aspirin 325 mg per day and clopidogrel 75 mg per day for 5 days prior to intervention. Alternatively, a clopidogrel loading dose of 300 mg can be administered 4 to 6 hours prior to the intervention.
■ Antihypertensive medications can be held off the day of intervention to prevent contribution to the possible periprocedural hypotension.
Positioning
■ The patient is placed in the supine position with adequate monitoring throughout the peri- and postprocedural period. Minimal monitoring includes continuous electrocardiogram (EKG), intraarterial blood pressure, and pulse oximetry. The patient’s neurologic status must be frequently evaluated during the procedure via answering of simple questions and squeezing a plastic sound toy (e.g., rubber duck squeaky toy) in the contralateral hand.
■ Intraarterial blood pressure monitoring is established usually via a radial arterial line.
■ In order to maintain patient cooperation/comfort and frequent neurologic monitoring, minimal or no sedation is administered and only local anesthesia is infiltrated for the access site.
TECHNIQUES
PERCUTANEOUS RETROGRADE FEMORAL ARTERY ACCESS
■ Obtain retrograde access via the common femoral artery (CFA) using a percutaneous micropuncture (21-gauge needle) system under ultrasound guidance. The CFA should be accessed immediately proximal to the femoral bifurcation in an area with minimal disease. The right CFA is the most convenient site for right-handed operators. The left CFA and brachial and radial arteries are alternative access sites. Ultimately, the safest and simplest access site to the target lesion should be employed.
■ The micropuncture sheath is then exchanged for a 5-Fr introducer sheath over the 0.035-in access wire.
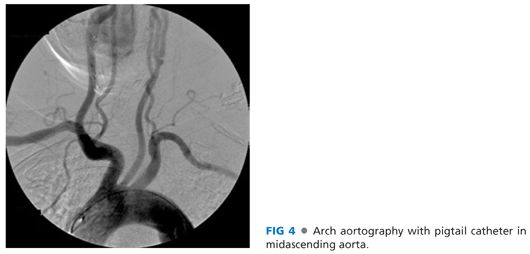
ARCH AORTOGRAPHY
■ A guidewire is advanced into the aortic arch followed by a pigtail catheter. The pigtail catheter is positioned in the mid-ascending aorta and arch aortography is performed in a 45- to 60-degree left anterior oblique projection in order to adequately visualize the origin of the great vessels (FIG 4).
SELECTIVE COMMON CAROTID CATHETERIZATION
■ Before further manipulation of wires/catheters in the arch and great vessel origins, the patient is administered systemic heparin at 70 to 100 U/kg intravenously (IV) with a goal activated clotting time of 250 to 300 seconds.
■ While maintaining the left anterior oblique (LAO) projection that allows for optimal visualization of the great vessels origins, a road map image is used to assist in selective catheterization of the CCA. The pigtail catheter is exchanged for the operator’s catheter of choice.
■ Multiple curved catheters are available (FIG 5), each with unique features that may be beneficial in different anatomies. However, frequently, selective common carotid catheterization can be accomplished with a combination of an angled or simple curved catheter and a floppy angled Glidewire™.

■ However, a retroflexed or complex curved catheter (e.g., SIM or Vitek) may be necessary with a difficult arch anatomy such as type III arch or bovine configuration (FIG 6).

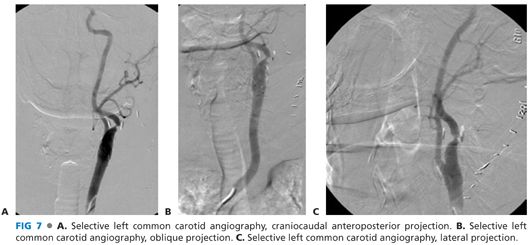
■ After the Glidewire™ has accessed the common carotid (but taking extreme care not to advance past the bifurcation), the selective catheter is advanced over the Glidewire™ into the common carotid. Common carotid–selective angiograms are then performed typically in the anteroposterior, lateral, and oblique projections (more views are performed as needed) (FIG 7). Contralateral carotid arteriogram can be performed as well if necessary, but this usually is not performed during CAS of a unilateral lesion.
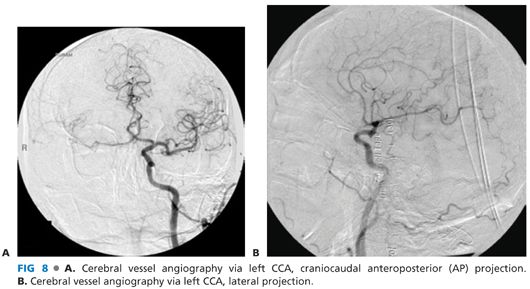
■ Cerebral vessel angiography is then performed, typically in anteroposterior and lateral views (FIG 8). Additional views can be done if necessary.
PLACEMENT OF GUIDING SHEATH
■ After common carotid angiography is complete, it is recommended that the appropriate necessary equipment to complete the procedure is selected prior to further selective cannulation of the carotid vessels (e.g., access sheaths, wires, catheters, filter and filter retrieval system, pre- and postdilatation balloons, stent).
■ In order to advance a sheath into the proximal common carotid, adequate exchange support is needed with a stiff guidewire. To achieve this, the selective catheter is carefully advanced over the floppy Glidewire™ into a branch of the external carotid artery (ECA). The floppy Glidewire™ is then exchanged for a stiff guidewire (e.g., long Amplatz™ Superstiff wire with floppy tip). Caution needs to be exercised to ensure the stiff wire tip does not inadvertently advance and potentially perforate the ECA branch. The catheter is then removed leaving the stiff wire in place in the ECA (FIG 9). If there is significant atherosclerotic stenosis involving the carotid bifurcation, or if the ECA is severely stenotic/occluded that prevents safe ECA access, an Amplatz™ wire with a 1-cm floppy tip may be left in the distal CCA.

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


