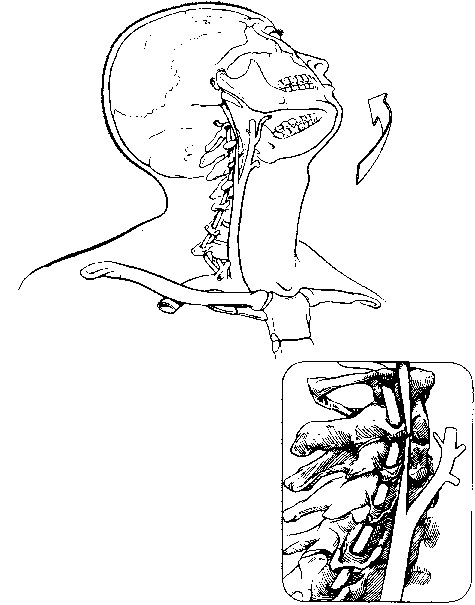
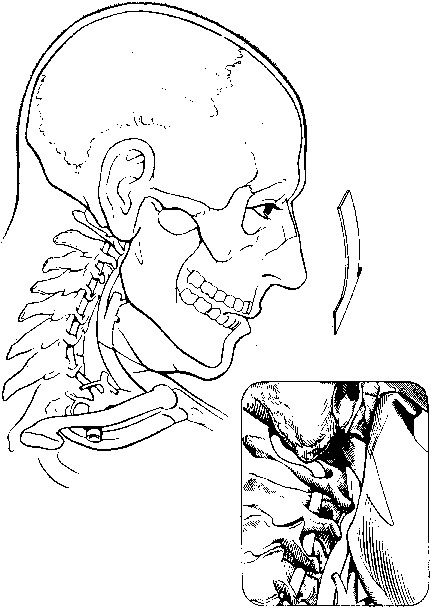
Carotid artery dissection can occur as a result of clear-cut stretch–traction–rotation injury (Figure 1) or direct compression between the angle of the jaw and the transverse vertebral processes (Figure 2). In the setting of significant trauma, such as a motor vehicle accident or a direct blow to the neck, cranial–cervical CT images are typically obtained and a rapid diagnosis follows. However, repetitive stress injury, whereby minor stresses of a subcritical nature accumulate and cause a dissection, is often associated with a delay in diagnosis. A number of precipitating events have been cited in case reports, including violent coughing, forceful emesis, heavy exercise, looking over one’s shoulder while driving, and chiropractic manipulation. Such reports are anecdotal at best. Intraoral trauma, typically in a child falling with a pencil or other object in his or her mouth, also has been reported. Certain diseased arteries, such as in patients with fibrodysplasia or connective tissue disorders, have a propensity to dissect. Many other arteriopathies and conditions are occasionally noted in conjunction with carotid artery dissections (Box 1).
Carotid Artery Dissections
Clinical Pathophysiology
Carotid Artery Dissections



