Cardiac Masses
The finding of a cardiac mass often has significant clinical implications and therefore apparent masses need careful echo evaluation to determine, as far as possible, their likely nature. Some harmless structures, such as the right ventricular (RV) moderator band, can give the appearance of a mass, and so it is particularly important to try to distinguish a mass that is pathological from one that is a normal variant. Cardiac masses on echo can result from:
tumours
primary cardiac tumours
benign
malignant
secondary cardiac tumours
thrombus
vegetations
normal variants and other conditions
moderator band
Lambl’s excrescences
Eustachian valve
Chiari network
lipomatous hypertrophy of the interatrial septum
dilated vessels
cysts
implanted devices.
TUMOURS
The echo assessment of a cardiac tumour should include a description of its:
size (measure its dimensions)
location
shape (e.g. spherical, pedunculated, papillary, flat)
surface appearance (e.g. regular, irregular, multilobular)
texture (e.g. solid, layered, cystic, calcified, heterogeneous)
mobility (mobile or fixed)
associated features (local invasion, pericardial effusion).
Because echo does not allow for a precise diagnosis, it is generally more appropriate to report a cardiac mass as being, for example, ‘suggestive of a myxoma’ than as a ‘definite’ myxoma.
The characteristics of the commonest tumours, and the features that distinguish them from other cardiac masses, are described below.
Primary cardiac tumours
Primary cardiac tumours are those that arise from the heart itself. They are rare (1 in 2000 autopsies) and 75 per cent are benign (Table 27.1).
Primary cardiac tumours can present with systemic features such as fever and weight loss, or more specifically with:
embolism – either of part the tumour itself or adherent thrombus
obstruction – usually of a valve orifice or outflow tract
arrhythmias – either tachyarrhythmias, such as ventricular tachycardia, or atrioventricular block.
However, cardiac tumours are most commonly discovered incidentally during echo studies for other indications.
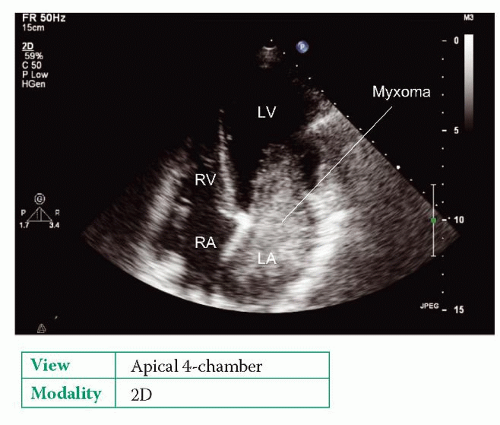
Myxoma
Myxoma is the commonest primary cardiac tumour, accounting for 50 per cent of cases, and is commoner in women. It is typically diagnosed between the ages of 30 and 60 years. Myxomas are usually (but not always) solitary: 75-80 per cent are found in the left atrium (LA, Fig. 27.1), 15-20 per cent in the right atrium (RA), and rarely in the ventricles.
Around 7 per cent of myxomas are familial (autosomal dominant), and these are more commonly multiple and found in the ventricles. Familial myxomas tend to present at a younger age. There can be associated abnormalities such as facial freckling and endocrine tumours, and such syndromes are grouped together as a ‘Carney complex’. Other myxoma syndromes include NAME syndrome and LAMB syndrome. Screening of first-degree relatives is appropriate in suspected familial cases.
Myxomas are attached to the heart by a pedunculated stalk – in the case of atrial myxomas, they attach to the interatrial septum at the fossa ovalis. The echo appearances of a myxoma are of a well-defined mass, which is often mobile, and the pedicle may be visible. The tumour itself appears heterogeneous and may contain small areas of lucency and occasionally speckles of calcium. Transthoracic echo (TTE) is usually adequate for making the diagnosis, but transoesophageal echo (TOE) has a greater sensitivity and specificity and provides a more detailed assessment of the myxoma.
Table 27.1 Primary cardiac tumours | ||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
|
 |
SAMPLE REPORT
The LA contains a mass attached to the interatrial atrial septum via a pedicle. The mass is approximately spherical, measuring 1.6 cm by 1.4 cm, and has an irregular surface and a heterogeneous texture with areas of lucency and of calcification. The mass is mobile but is not causing any obstruction to mitral valve flow. No other intracardiac masses are seen. The appearances are suggestive of a left atrial myxoma.
Surgical resection of the myxoma is the treatment of choice. Following resection, longer-term follow-up is appropriate to monitor for tumour recurrence (particularly in familial cases, where the recurrence rate is 20 per cent).
Other benign cardiac tumours
Papillary fibroelastoma is a small (<1.5 cm) benign tumour and is most commonly found attached to the aortic or mitral valve. They account for 10 per cent of primary cardiac tumours. They are usually found incidentally during echo, cardiac surgery or post mortem, and their similarity to vegetations can lead to a mistaken diagnosis of infective endocarditis. They are usually highly mobile and have been described as having a ‘shimmering’ appearance around the edges on echo. The tumours can be a source of thrombotic emboli, or fragments of the fibroelastoma itself can embolize, and surgical resection should therefore be considered, particularly if they are large (>1.0 cm), mobile and present in the left heart.
Lipomas are usually seen beneath the epicardium. Cardiac magnetic resonance imaging (MRI) is a useful technique to confirm the diagnosis. Lipomas are distinct from lipomatous hypertrophy of the interatrial septum (see below).
Haemangioma is a rare benign vascular tumour which can occur in any chamber.
Rhabdomyoma is the commonest cardiac tumour seen in infants and children. It is usually multiple and found in the ventricles. It is commonly associated with tuberous sclerosis.
Fibromas are also commonest in infants and children, are usually solitary, and mainly affect the interventricular septum. Fibromas are up to 10 cm in diameter
and appear heterogeneous with multifocal calcification on echo. They often cause obstruction and arrhythmias.
and appear heterogeneous with multifocal calcification on echo. They often cause obstruction and arrhythmias.
Teratomas are germ cell tumours found in infants and children that usually affect the pericardium and are associated with a pericardial effusion. Echo shows a complex cystic mass within the pericardium and usually on the right side of the heart.
Malignant primary cardiac tumours
Malignant tumours make up 25 per cent of primary cardiac tumours and the vast majority are sarcomas. There are various types of cardiac sarcoma, including angiosarcoma (the commonest), rhabdomyosarcoma, malignant fibrous histiocytoma and osteosarcoma.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


