The Left Atrium
The left atrium (LA) can be thought of as having three key haemodynamic functions. During left ventricular systole and its subsequent isovolumic relaxation phase, the LA acts as a reservoir for oxygenated blood returning to the heart from the lungs. During early diastole, the LA then acts as a passive conduit for this blood to enter the left ventricle. In late diastole, atrial contraction actively boosts left ventricular filling (unless the patient is in atrial fibrillation).
ECHO ASSESSMENT OF THE LEFT ATRIUM
The left atrium (LA) can be seen in several views:
left parasternal window
parasternal long axis view
parasternal short axis view (aortic valve level)
apical window
apical 4-chamber view
apical 2-chamber view
apical 3-chamber (long axis) view
subcostal window
subcostal long axis view.
An echo evaluation of the LA includes assessment of:
LEFT ATRIAL MORPHOLOGY
Inspect the overall size and shape of the LA, and check for the presence of any masses (e.g. tumour, thrombus). Be alert too for the presence of spontaneous echo contrast, particularly in presence of atrial fibrillation and/or mitral stenosis. Although best seen on transoesophageal echo, spontaneous echo contrast may also be evident during transthoracic imaging. LA masses and spontaneous echo contrast are discussed further in Chapter 27.
The left atrial appendage is not easily seen on transthoracic echo, but may be visible in the apical 2-chamber view. The pulmonary veins can sometimes also be hard to spot, but are generally best seen in the apical 4-chamber view (especially the right upper pulmonary vein, Fig. 17.3).
COR TRIATRIATUM
Cor triatriatum is a rare congenital abnormality in which the LA is partitioned into two chambers by a membrane, best seen in the apical 4-chamber view. The membrane contains one or more perforations allowing blood to flow between the two chambers, but nonetheless there is a degree of obstruction to LV inflow which can be assessed using PW Doppler. Cor triatriatum dexter is the name given to this condition when it occurs in the right atrium.
LEFT ATRIAL DIMENSIONS
mitral valve disease
dilated cardiomyopathy
restrictive cardiomyopathy
LV diastolic dysfunction
atrial fibrillation or flutter
high-output states (e.g. anaemia)
‘athlete’s heart’ (p. 245).
LA diameter is measured at end-systole in the parasternal long axis view, using either 2D or M-mode imaging (Fig. 18.2).
LA volume is measured using the modified Simpson’s rule method:
1. In the apical 4-chamber view obtain the best view you can of the LA, paying particular attention to avoidance of foreshortening.
2. Freeze a loop and find the end-systolic image. Now trace the endocardial border around the LA to obtain an area measurement in cm2. Ignore any pulmonary veins that may be visible.
3. Measure the length of the LA long axis in cm from the mid-point of the mitral annulus to the superior border (back wall) of the LA.
4. Repeat the measurements in the apical 2-chamber view.
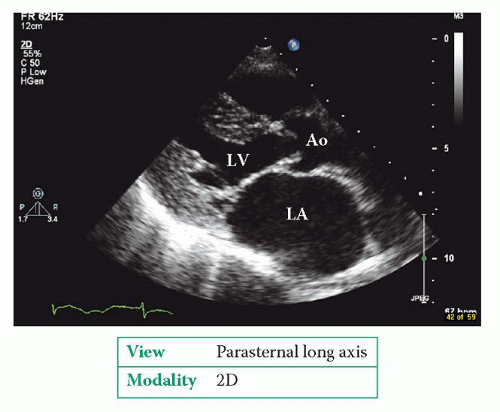 Figure 18.1 Dilated left atrium (LA
Get Clinical Tree app for offline access
Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree


|