We are interested in the recent meta-analysis by Singh et al concerning takotsubo cardiomyopathy (TTC) as it relates to cardiac arrest. Obviously, the investigators of that study, by retrospectively reviewing short series and single case reports, could not obtain definitive data about “the natural history” of this disease entity. However, their review was, indeed, important to clarify some current information regarding the mechanisms and incidence of cardiac arrest in TTC.
We would like to point out the following facts about this rare and puzzling syndrome:
- 1.
Most likely, most deaths after the onset of TTC occur in the very early stage of an event. Unfortunately, this phase is rarely witnessed by physicians; it generally occurs outside the hospital, lasts for only a few minutes, and has a high mortality rate. Cases that occur in the hospital may be more revealing than those in which the patient is admitted to the hospital 1 to 12 hours after the onset of TTC.
- 2.
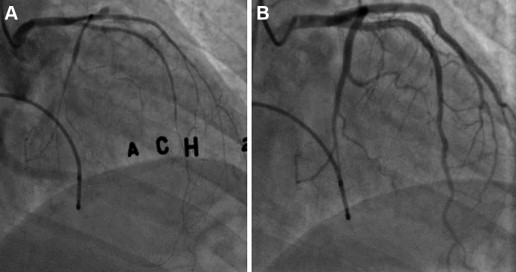
In studying the mechanism and consequences of TTC, the best available evidence is derived from clinical experimentation aimed at reproducing TTC during the recovery phase. The best technique for this purpose is acetylcholine (ACH) testing of endothelial dysfunction. In a significant percentage of patients recovering from TTC, ACH testing reveals severely increased spasticity of many epicardial branches in the TTC-affected area, which frequently leads to reproduction of the original segmental myocardial dysfunction ( Figure 1 ). Often, total occlusion is elicited by routine ACH test doses, and this is the time when the risk is highest for the onset of ventricular fibrillation. If given early, intracoronary nitroglycerin infusion consistently and immediately resolves the spastic responses (coronary and myocardial). In our short series, we have seen both cardiac standstill and ventricular tachycardia, but no patient has required electrical cardioversion, and spasm has persisted only for 30 to 60 seconds. Rarely can such early coronary spasm be documented at the time of these patients’ admission to the hospital, but the theory that spasm is responsible for inducing TTC myocardial stunning and arrhythmias is quite compelling, even on the basis of our early, single-center experience. The condition is not inducible in every TTC patient. In fact, an episode of TTC seems to induce immunity, by an unknown mechanism, consistent with clinical experience (5% to 10% probability of recurrence). Our attempt to co-ordinate a multicenter prospective study is encountering serious difficulties, mainly because many clinicians believe that the catecholamine/stress theory is correct and adequate; however, this theory has never been proved, catecholamine levels in TTC are not usually tested, and only ∼5% of pheochromocytoma patients have TTC.