Bullous Disease of the Lung
DEFINITION
A bulla is an air-containing space within the lung parenchyma that arises from destruction, dilatation, and confluence of airspaces distal to terminal bronchioles and is larger than 1 cm in diameter (Fig. 52-1).1 Its walls are composed of attenuated and compressed parenchyma. Bullae occur in various clinical contexts: (1) with emphysema (“bullous emphysema”); (2) with pulmonary fibrosis, as in the late stages of sarcoidosis or complicated pneumoconiosis; (3) in so-called “vanishing lung,” in which the parenchyma is rapidly replaced by multiple bullae; and (4) in lungs that are otherwise normal (“bullous lung disease”) and, therefore, likely secondary to a mechanism different from that of bullae occurring in conjunction with emphysema (Table 52-1).2,3
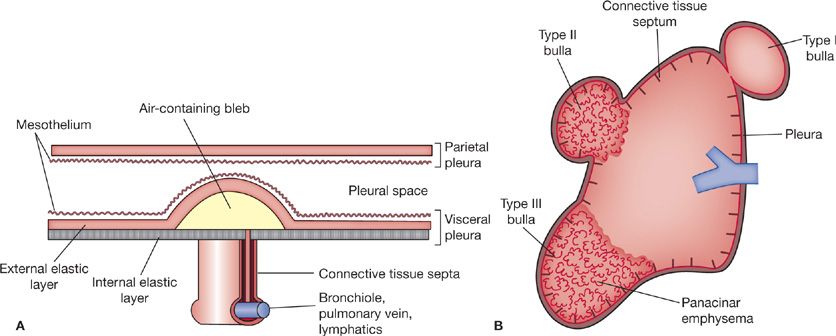
Figure 52-1 Blebs and bullae. A. Development of a bleb. A bleb is an accumulation of air within the pleura that is not confined by connective tissue septa within the lung. Air that escapes within the substance of the lungs makes its way to the surface, separating the internal from the external elastic layers on the visceral pleura. B. Different types of bullae. In contrast to a bleb, a bulla is confined by connective tissue septa of the lung and is deep to the internal elastic layer of the visceral pleura. Three different types of bullae are shown arising from a lung that has been removed from within the chest wall. A type I bulla is shown at the apex, a type II is in the middle zone, and a type III is arising at the base. The short dark lines denote connective tissue septa. Panacinar emphysematous parenchyma is present within the types II and III bullae. (Adapted with permission from Reid L. The Pathology of Emphysema. Chicago: Year Book; 1967:211–240.)
Distinctions are drawn between bullae, blebs, and cysts (Table 52-2).2 A bleb is an accumulation of air between the two layers of the visceral pleura that arises when the thin covering of the bleb ruptures and permits entry of air (Fig. 52-1). Cysts are epithelial-lined cavities that may resemble bullae on radiographs.3 Many fall into the category of developmental anomalies and include mixtures of mesenchymal and epithelial components that are normally present in the lung. The pathologic nature of these cystic lesions is reflected in their names: “cystic adenomatoid malformations,” “peripheral bronchogenic cysts,” “congenital polycystic disease,” and “atypical bronchopulmonary sequestration.”1
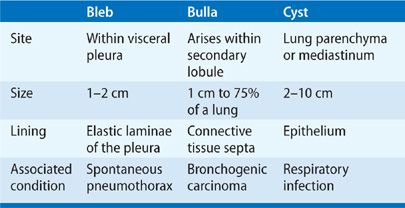
The term bullous disease is reserved for multiple bullae in lungs that are otherwise normal.2 This entity is different in etiology and pathogenesis from that in which bullae occur in conjunction with underlying chronic obstructive pulmonary disease (COPD). Confusion occasionally arises between the two entities because some pathologists regard bullous disease as a subset of panacinar emphysema.1 However, this view is not useful as (1) panacinar emphysema tends to occur in the lower lobes, whereas bullous disease favors the upper lobes; (2) the natural history of the two disorders is quite different; and (3) panacinar emphysema has certain distinctive features not shared by bullous disease. Bullae may occur not only as part of obstructive lung disease, but also as a complication of fibrotic lung disease (Table 52-1).
ETIOLOGY
Bullae may originate in a variety of clinical and pathogenetic settings: (1) with emphysema of distal acini; (2) in the setting of cigarette smoking; (3) in conjunction with scar tissue formation, which “traps” areas of normal lung, enlarges airspaces by traction on surrounding intact alveoli, or produces retraction or shrinkage of intact walls of adherent alveoli; (4) in the setting of intravenous drug abuse; (5) as a result of chronic inflammation and destructive changes in terminal and first-order respiratory bronchioles, resulting in airspace distention from delayed emptying; and (6) with α1-antitrypsin deficiency.2,4,5
CLASSIFICATION
Bullae are classified anatomically into three main types (Fig. 52-1B).1,2 Type I bullae are characterized by a narrow neck that connects the bullae with the pulmonary parenchyma. This type of bulla may be caused by overinflation of a volume of flawed lung tissue. The walls of type I bullae are thin, and their interiors are empty. Type I bullae are usually found at the lung apices and along the edges of the lingula and middle lobes. They often occur in association with paraseptal emphysema. Scanning electron microscopy has demonstrated that the thin neck is a consistent feature and that pleural mesothelial cells on the external surface are either reduced in number or completely absent; bundles of collagen fibers lie naked and separated from one other by small pores or crevices.
Type II bullae arise from the subpleural parenchyma and are characterized by a neck of panacinar emphysematous lung tissue. The interior of these airspaces consists of emphysematous lung in which blood vessels are still present. In contrast to type I bullae, the outer wall is formed by pleura covered with intact mesothelial cells. Although connective tissue septae are present within the bullae, they are not found in the wall. Type II bullae may occur anywhere in the lung, but they are most frequent in the upper lobe, at the anterior surface of the middle lobe, and over the diaphragm.
Type III bullae consist of slightly hyperinflated lung connected to the rest of the lung by a broad base extending deep into the parenchyma. This type is believed to represent an atrophic form of emphysema.
PATHOGENESIS
Several hypotheses have been proposed over the years for how bullae develop, although none have been proved.1,2,3,6 These include (1) weakness of the alveolar walls predisposes to the formation of bullae, particularly at the apices of the lungs, where pleural pressures are most negative. This theory underscores the proclivity of bullae for the upper lobes and stresses the influence of mechanical forces acting upon flawed tissue. (2) Inflammatory disease of a bronchiole leads to progressive air trapping and “tension airspaces.” (3) Disordered collateral ventilation produces the findings. (4) The same mechanisms responsible for generalized emphysema are operative in the formation of bullae. (5) Underlying paraseptal emphysema produces bullous disease.
Of all the hypotheses, that of underlying paraseptal emphysema is the most popular.1,2 The hypothesis envisages destruction of alveoli adjacent to connective septae or the pleura. The pattern relates to the fact that capillaries in alveolar walls that abut connective tissue septa are less numerous than elsewhere because of a sparse network of arterioles and arteries in peripheral alveoli. Consequently, these regions of the acinus have less vascularity and greater compliance.
Dynamic computerized tomography and intrabulla pressure measurements have raised questions about the theory that bullae are formed by positive pressure within the airspace.1,7 The lung surrounding a bulla is less compliant than the bulla itself; accordingly, the pressure necessary to inflate the surrounding lung is greater than that necessary to inflate the bulla. The pressure within a giant bulla has been found to be the same as pleural pressure. Therefore, when a bulla and its surrounding lung are exposed to the same negative pleural pressure, the bulla fills preferentially and completely like an inflated paper bag, prior to the surrounding lung inflating. Further inspiration increases the elastic recoil pressure, thereby exerting a greater retractive force on the lung parenchyma and enlarging the airspace. Nevertheless, bullae can be removed from within the lung while still maintaining their volume, indicating a positive intrabulla pressure.
Bullae within the intact chest are molded and compressed to fit adjacent anatomic configurations. However, if the lung is released from these constraints (e.g., when removed from the chest cavity), bullae project as shiny bubbles at the lung surface (Fig. 52-2). Within the thoracic cavity, large bullae cause crowding of adjacent lung parenchyma, and structures such as bronchi are displaced, stretched, and narrowed over the bullae surfaces. Very large airspaces can expand across the midline or even extend into the neck. Bullae represent more than just overexpanded alveoli, because the remnants of bronchioles and their accompanying vessels sometimes persist as trabeculae within the bullae. Interlobular septae can be incorporated into the wall as the airspace expands from within the secondary lobule.
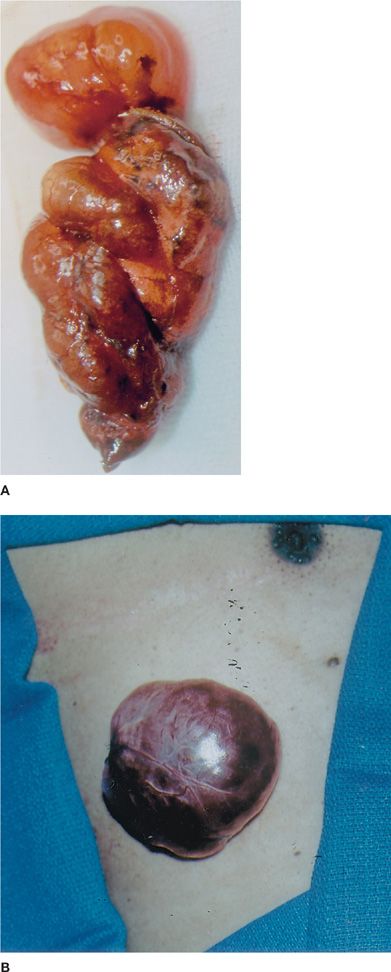
Figure 52-2 A. Surgically resected specimen with a bulla projecting from the lung surface. B. A bulla is shown projecting through a previous chest tube insertion site onto the surface of the skin.
Two important risk factors for bullous emphysema are cigarette smoking and α1-antitrypsin deficiency. Many patients with bullous emphysema are cigarette smokers, and most bullous lesions are associated with paraseptal or centriacinar emphysema. Although bullous emphysema is typically found in young males, elderly patients with α1-antitrypsin deficiency who are lifelong nonsmokers may develop bullous changes in later life. A hereditary predisposition to bullous emphysema is also suggested by its association with a variety of rare familial disorders, including Fabry disease, Salla disease, cutis laxa, Ehlers–Danlos syndrome, and Marfan syndrome.1 Giant bullous emphysema has also been reported with histologic changes of placental transmogrification—a rare, benign lung disease of unknown etiology in which the lung shows bullous changes or, rarely, cysts or nodules.8,9 Lung pathology demonstrates papillary structures similar to placental villi surrounding the pulmonary epithelium. The tight skin mouse, which has a dominant mutation for the elastase gene and is characterized by multiple connective tissue abnormalities, serves as a unique model for bullous emphysema.10
DISTRIBUTION OF BULLAE
As noted previously, the tendency for bullae to occur in the upper lobes is usually attributed to the greater mechanical stresses imposed on the lung apices than bases. Because intrapleural pressure near the lung apices is more negative than at the bases, apical alveoli are subjected to greater expanding stresses than are basal alveoli. Radioactive gas studies and in situ freezing techniques have demonstrated that alveoli in the upper lung zones are considerably larger than those in the lower zones. Gravity also plays a role, as the upright lung behaves like a coiled spring, which, when allowed to dangle in the upright position, shows larger gaps between coils at the top than the bottom.
Engineering techniques used to study the distribution of stresses in aircraft have been applied to the analysis of stresses on the lung.1 These have shown that the larger expanding stresses at the apices are directed primarily in a vertical direction, and to a lesser extent, laterally. The stresses tend to increase with expansion of the lung, but they are present also when the lung volume decreases below functional residual capacity (FRC). The increase in apical stress at low lung volumes has been attributed to an increase in the rigidity of the lungs as residual volume is approached.
EVALUATION AND DIAGNOSIS
In asymptomatic individuals, bullae may be detected in the course of routine chest radiography. Small bullae rarely become visible on the chest radiograph but are usually easily visible by computed tomography (CT). As a rule, small bullae usually produce no symptoms, signs, or discernible alterations in pulmonary function.11 However, rupture of one or more bullae may lead to spontaneous pneumothorax (see below). In some patients bullae give rise to progressive dyspnea or chest pain (Fig. 52-3A,B).12 On occasion, a patient with bullous lung disease develops sudden, severe breathlessness secondary to development of a spontaneous pneumothorax13 or sudden increase in bulla size due to air trapping. In patients with known bullous disease infection in a bulla can occur (see below). Radiographically, infection is usually identified by the appearance of an air–fluid level (Fig. 52-4A).4–6 The physical findings in a patient with one or more bullae usually reflect the overall state of the lungs. Only infrequently do giant bullae reach a size sufficient to cause a localized decrease in regional air entry, with absent breath sounds and increased resonance to percussion.
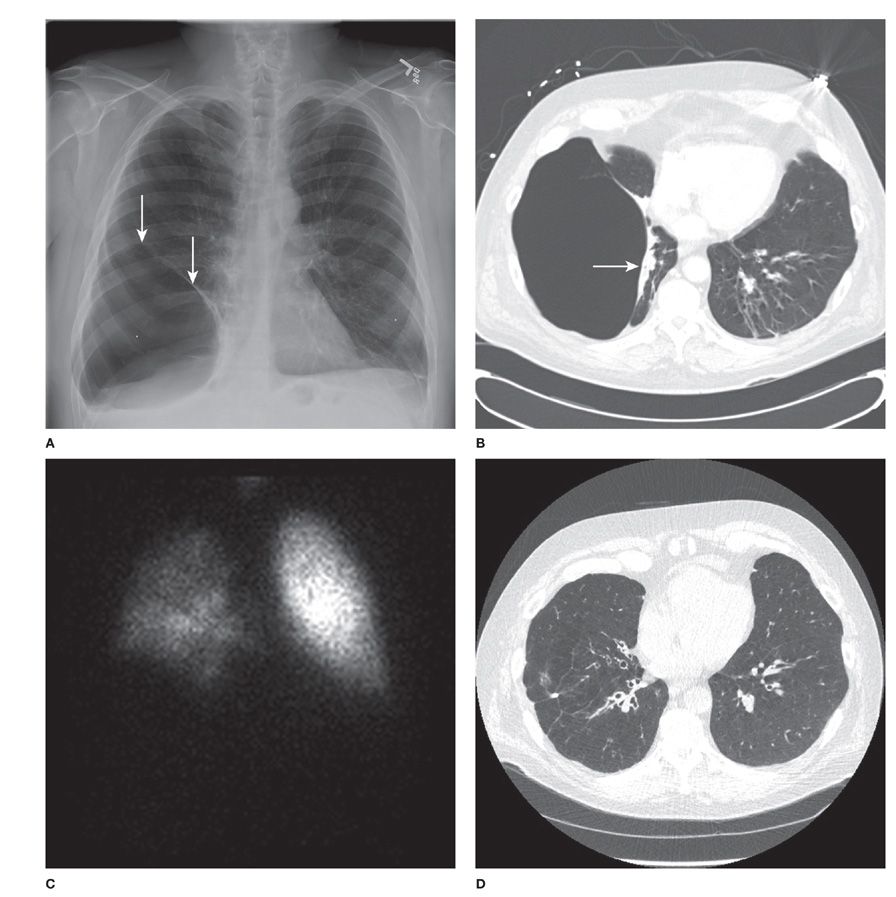
Figure 52-3 A. Chest radiograph demonstrating a right lower lobe bulla. Note the demarcating lines, or “hairline shadows” (arrows). B. CT image of the lungs demonstrating the right lower lobe bulla with compressed lung (arrow). C. Perfusion scintigraphy demonstrating decreased perfusion to the right lower lung zone. D. CT image of the lung following surgical resection of the right lower lobe bulla.
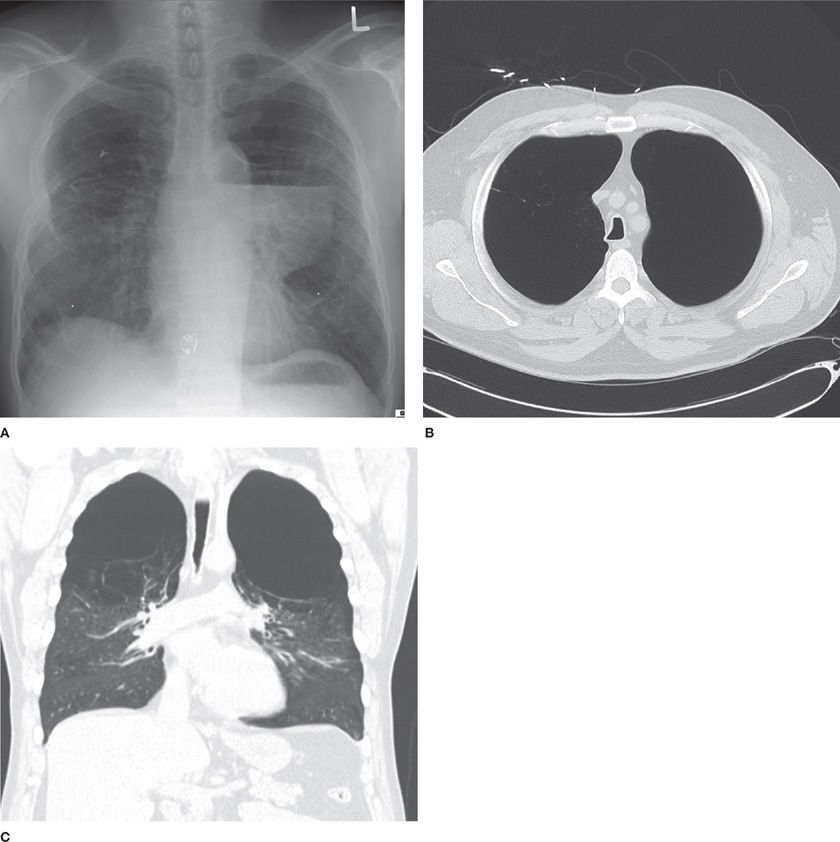
Figure 52-4 A. Chest radiograph (PA view) showing bilateral upper zonal areas of increased radiolucency and an air-fluid level in the left upper lobe bulla. B. Chest CT scan (axial view) demonstrating bilateral upper lobe bullae. C. Chest CT scan (coronal view) demonstrating bilateral upper lobe bullae.
 LABORATORY
LABORATORY
Routine laboratory testing in the evaluation of bullae includes the measurement of hemoglobin and hematocrit to identify if anemia is contributing to respiratory symptoms and to assess for possible secondary polycythemia due to chronic hypoxemia.1,12 Measuring an α1-antitrypsin level should be obtained to diagnose α1-antitrypsin deficiency.14 Finally evaluation of arterial blood gases, performed while the patient is breathing room air if possible, is generally indicated in patients with severe respiratory insufficiency and those being evaluated for possible bullectomy.12 As noted in Table 52-3, a PaC2 greater than 45 mm Hg is considered a relative contraindication for bullectomy.15
 IMAGING
IMAGING
Imaging techniques used in the evaluation of bullous lung disease include chest radiography, computed tomography, and nuclear medicine-based studies.
Chest Radiography
Although routine chest radiography is the most practical method for identifying the presence of bullae, the technique generally discloses less than 50% of bullae identified on CT.16,17 In a given patient, serial radiographs taken over years are invaluable in tracing evolution of the disease.11 The presence of the condition is suggested by areas of increased radiolucency that are sharply delineated by fine radiopaque lines representing the walls of the bullae. These lines, or “hairline shadows,” are composed of compressed and fused interlobular septae or pleura.10,18 Because the hairline shadows appear incomplete on the chest radiograph, they delineate only segments of the bulla wall (Fig. 52-3A). Distinction between hairline shadows produced by a bulla, and thicker, sometimes irregular, walls of a cavity is usually not difficult. More difficult is distinguishing bullae from cysts. The presence of other radiologic signs of emphysema or fibrotic lung disorders suggests that the cystic structure is a bulla.13 Similarly, distinguishing between a large bulla and pneumothorax may be challenging.12,19 In general, the pleural line associated with a large bulla is usually concave relative to the lateral chest wall, whereas the pleural line associated with a pneumothorax is convex relative to the lateral chest wall.12 Similarly observation of “the double-wall sign” (i.e., the presence of air on both sides of the bulla wall) may be helpful in identifying the findings as due to a bulla.18
A chest radiograph obtained after forced expiration is sometimes helpful in demonstrating the presence of bullae: air trapping during the expiratory maneuver accentuates their outline by preventing a decrease in their size as the surrounding lung empties.3 Large bullae sometimes displace the mediastinum contralaterally and may even compress the opposite lung.
Computed Tomography
CT provides valuable anatomic information about the size, number, and relationships of bullae, as well as crowding of adjacent lung and disposition of the pulmonary vasculature (Fig. 52-3B).20–22 Bullae are identified as areas of radiolucency that usually do not contain blood vessels and that are confined by visible walls. High-resolution computed tomography (HRCT) shows that large bullae are frequently associated not only with distal acinar (paraseptal) emphysema, but also with centriacinar emphysema—the type of emphysema usually associated with cigarette smoking.20
These observations are consistent with the hypothesis that peripheral airspaces in paraseptal emphysema may coalesce to form larger bullae that may crowd normal adjacent lung. In addition, CT has shown that when bullae occur in the context of generalized emphysema, the extent of bullous emphysema correlates poorly with measurements of pulmonary function, and that the main determinant of respiratory function is the severity of emphysema in the bullous-free parts of the lung.23
On chest CT, giant bullae are predominantly located in the upper lobes and are generally subpleural.12 However, in patients with α1-antitrypsin deficiency, bullae are most commonly located at the lung bases. Approximately half of the patients have bilateral bullae (Fig. 52-4), and, occasionally, deviation of the mediastinal structures to the contralateral side may be noted.12 CT has been used to create three-dimensional reconstructions of bullae, which can then be used to calculate bullae volumes (Fig. 52-5).
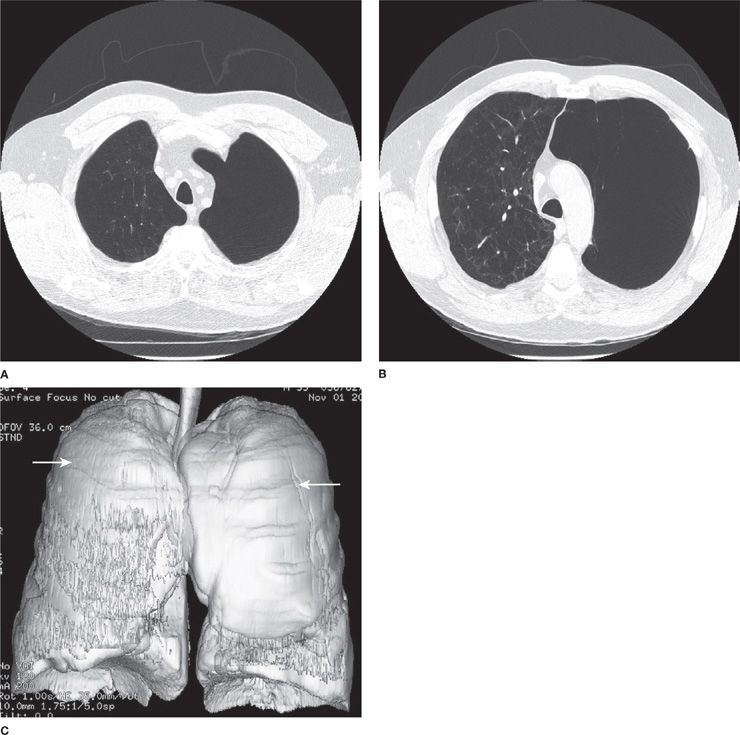
Figure 52-5 A. Chest CT (axial view) showing bilateral upper lobe bullae. B. Chest CT (axial view) demonstrating larger left upper lobe compared to right upper bulla. C. Chest CT (coronal view; three-dimensional reconstruction) demonstrating bilateral upper lobe bullae (arrows).
Nuclear Imaging
Lung scanning using radionuclide-based techniques may provide useful preoperative information in evaluating patients with bullous lung disease.24 A lung perfusion scan provides a semiquantitative assessment of regional blood flow (Fig. 52-3C); results of ventilation scans vary with the technique. A single-breath scan using 133xenon often fails to demonstrate ventilation of a bulla, whereas a continuous ventilation scan often shows slow filling and emptying of the structure.24,25 Complete lack of communication between the airways and bulla is reflected in the absence of filling during all phases of the continuous ventilation scan.
 PULMONARY PHYSIOLOGY
PULMONARY PHYSIOLOGY
Clinical evaluation of bullous lung disease is aided by assessment of pulmonary function, pulmonary mechanics, exercise performance, and the pulmonary circulation.
Pulmonary Function Tests
Pulmonary function tests have considerable practical value in distinguishing between individuals with localized bullae in whom intervening lung is normal (bullous disease), and those in whom localized bullae are part of obstructive airways disease (bullous emphysema) (Table 52-4).12 The distinction is important, since those with obstructive airways disease are generally poor surgical candidates because of impaired pulmonary function.



