Figure 11.1
Apical 4 chamber view of patient with an atrioventricular canal defect showing ostium primum atrial septal defect (thick arrow) and corresponding inlet ventricular septal defect (VSD-thin arrow), Please note that the valve (which is a common valve) appears as if mitral and tricuspid valves are on the same level

Figure 11.2
Apical short axis view showing a common valve in a patient with atrioventricular canal defect. SBL superior bridging leaflet, IBL inferior bridging leaflet, LLL left lateral leaflet, RSL right superior leaflet, RLL right lateral leaflet
defect in the group of atrio-ventricular septal defects appearing due to failure of septum primum fusion with endocardial cushion.
associated with AV valve malformation, cleft mitral valve and ventricular septal defects.
due to complexity of the lesion it will not be discussed in this section.
Ostium secundum atrial septal defect (Fig. 11.3, Video 11.3)
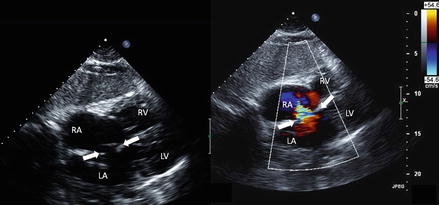
Figure 11.3
Subcostal views showing large ostium secundum atrial septal defect on the left (arrows) and shunt on the right (arrows)
results from either poor growth of septum secundum or increased absorption of septum primum during early stages of development
most common form of ASD
commonly found in central portion of the septum surrounding foramen ovale.
as left atrial pressures are higher than right atrial pressures, there is usually a left to right shunt early in the course of ASD which may stop and reverse the direction if pulmonary hypertension appears in cases of large shunts.
TTE and TEE are useful in evaluation of size of the defect, it’s location and feasibility of percutaneous device closure. Intraprocedural TEE is an essential part of percutaneous closure of secundum ASD (Fig. 11.4)
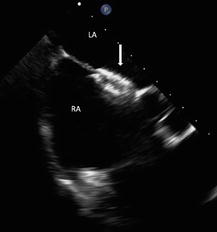
Figure 11.4
Transesophageal Echocardiographic view showing an Amplazer atrial septal defect closure device (the arrow)
Sinus venosus septal defects (Fig. 11.5)
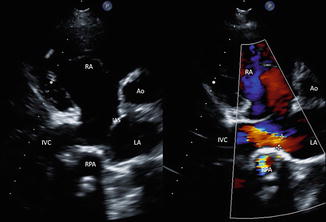
Figure 11.5
Right parasternal view showing Inferior Sinus Venosus Atrial Septal Defect with (right image) and without (left image) color Doppler. The jet of ASD is seen between 2 cross signs on the right image. IVC inferior vena cava, IAS interatrial septum, RPA right pulmonary artery, Ao aorta
Are divided in superior and interior
Occur due to abnormal insertion of superior or inferior vena cava (thus located in superior and posterior and inferior and posterior locations, respectively)
Frequently associated with partial anomalous venous return
Coronary sinus septum defect
Very rare
Occurs due to incomplete formation of atrio-venous fold
Often associated with persistent left superior vena cava
Interesting fact: Scimitar syndrome: Combination of hypoplastic right lung, hypoplastic pulmonary artery, and anomalous arterial blood supply to the right lung and characteristically curved right pulmonary vein draining into inferior vena cava. The name appears due to radiographic resemblance of anomalous venous return to the shape of Middle-Eastern sword scimitar.
Echocardiographic assessment of ASDs:
Type of defect
Location
Size
Shunt ratio calculation
Assessment of RA, RV
Assessment of PHTN
Imaging assistance in device closure of ASD.
Ventricular Septal Defects (VSD)
Interesting fact: Ventricular septal defect was originally reported by Dr. Dalrymple in 1847. Glazbrook AJ. Eisenmenger’s complex. Br Heart J. 1943;5:147–151
VSDs are separated anatomically into muscular, membranous, supracristal, and inlet.
VSDs may be congenital or acquired (s/p myocardial infarction)
Get Clinical Tree app for offline access
(a)
Muscular VSD (Fig. 11.6, Videos 11.4 and 11.5)
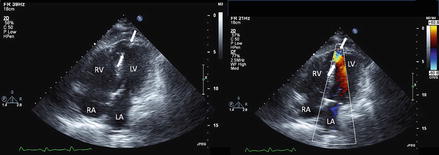
Figure 11.6
Off-axis apical four chamber views showing muscular VSD (arrows)
Most common VSD in neonates
90 % resolve within first year of life
(b)
Membranous VSD (Figs. 11.7 and 11.8)
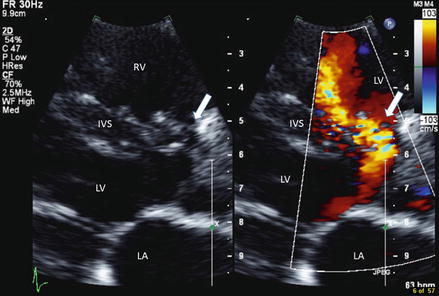
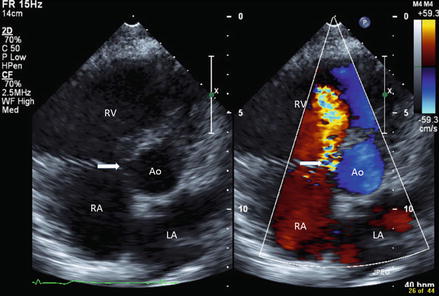
Figure 11.7
Parasternal long axis views showing membranous VSD (arrows). IVS interventricular septum
Figure 11.8
Parasternal short axis view showing membranous VSD (arrows). Please note dilated right ventricle
Also known as perimembranous
Most common type of VSD outside of infancy
(c)
Supracristal VSD (Figs. 11.9 and 11.10)
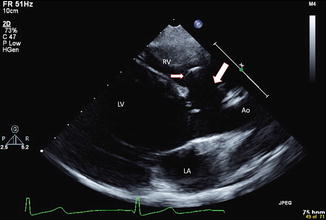
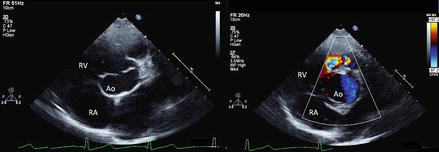
Figure 11.9
Parasternal long axis view showing patient with supra-crystal (cono-septal) VSD (large arrow) with aortic valve leaflet prolapse in the VSD (small arrow)
Figure 11.10
Parasternal short axis view showing patient with supra-crystal VSD and aortic leaflet prolapse. The right image shows the color Doppler image of the shunt
sometimes called subpulmonic
deficiency in the septum above and anterior to the crista supraventricularis beneath the aortic and pulmonary valves
lacks structural support of the right and/or the left aortic coronary cusp
may cause cusp prolapse through the defect leading to aortic regurgitation (which is often progressive over time)
(d)
Inlet VSD (Fig. 11.1)




sometimes called atrioventricular canal type VSD
associated with atrioventricular canal defects< div class='tao-gold-member'>Only gold members can continue reading. Log In or Register to continue
Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
