Chapter 15 Atrial Septal Defect
Simple and Complex
Galen was aware of the foramen ovale and its normal postnatal closure.1 Botallo described a patent foramen ovale after birth without understanding its function in the fetus.1 Leonardo da Vinci wrote, “I have found from left auricle to right auricle the perforating channel.” Leonardo’s account of a true atrial septal defect is thought to be the first record of a congenital malformation of the human heart.2 In 1640, Pierre Gassendi based an entire treatise on observations of a patent foramen ovale in an adult cadaver.3
Karl von Rokitansky, in 1875, published superb observations on the pathologic anatomy of atrial septal defects and what he presumed to be their embryologic basis and distinguished septum primum from septum secundum defects. In 1921, Assmann’s4 description of the radiologic features of atrial septal defects paved the way for clinical recognition. In 1934, Roesler5 analyzed 62 necropsy cases of atrial septal defect, only one of which had been correctly diagnosed during life. In a landmark publication in 1941, Bedford, Papp, and Parkinson6 described the clinical features of atrial septal defects. Hudson’s7 1955 description of the normal and abnormal interatrial septum was refined in 1979 by Sweeney and Rosenquist.8 These early accounts have been extended by studies of the anatomy of the interatrial septum with tranesophageal echocardiography.9
The normal atrial septum viewed from its right side is a blade-shaped structure with a superoanterior margin that reflects the curvature of the ascending aorta, an inferior margin that borders the mitral annulus, and a posterior margin that is convex.8 The left side of the septum has a network of trabeculations that are remnants of the septum primum.
The fossa ovalis occupies about 28% of the septal area, irrespective of age, and is bordered by a limbus and guarded by a valve (see Figure 15-46C).8 After birth, the patent fetal foramen ovale closes via fusion of its valve with the limbus of the fossa ovalis as left atrial pressure exceeds right atrial pressure. The incidence of persistent patency of the foramen ovale declines from about one third during the first three decades of life to about one quarter during the fourth through eighth decades.10 The morphogenetic sequence of normal intrauterine formation and closure of the atrial septum is illustrated in Figure 15-1.7 Redundancy of the valve of the foramen is responsible for an atrial septal aneurysm (see Figure 15-47).11,12
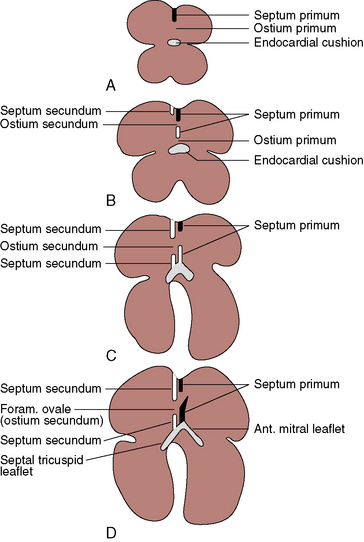
The most common type of atrial septal defect is in the ostium secundum or fossa ovalis location (Figures 15-2 and 15-3).13–15 These defects lie in a folded area rather than on a flat plane. Their anatomy is more complex on the right side than on the left side of the septum.16 Ostium secundum defects result from shortening of the valve of the foramen ovale, excessive resorption of the septum primum, or deficient growth of the septum secundum (see Figures 15-1, 15-2, and Figure 15-46C). Occasionally, the atrial septal perforations resembles Swiss cheese,17 or the interatrial communication is represented by multiple openings less than 5 mm in diameter.18
Next in frequency are ostium primum defects, also called atrioventricular septal defects because the atrioventricular septum is defective (absent; see Figures 15-1 and 15-2). Oddly and rarely, a communication exists in the atrioventricular septum when septal structures are intact.19
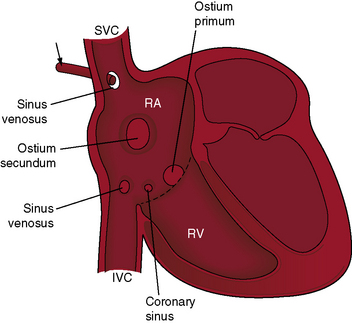
Sinus venosus atrial septal defects are uncommon, but not rare, and constitute 2% to 3% of interatrial communications. During normal embryogenesis, the inferior vena cava and the right superior vena cava are incorporated into the right horn of the sinus venosus. Faulty resorption results in a communication near the orifice of the superior or the inferior cava. The right valve of the sinus venosus is a broad membrane that almost partitions the developing right atrium. Both vena cavas are located on the left side of the membrane. The principle type of sinus venosus defect was described in 1868 as a “free communication between the auricles by deficiency of the upper part of the septum auricularum.”20
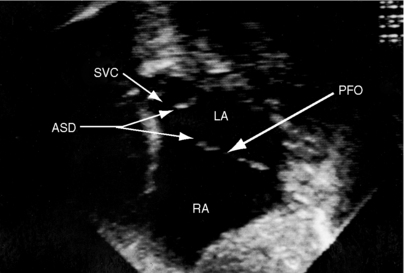
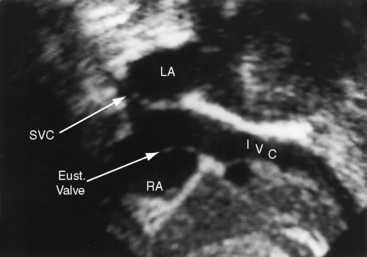
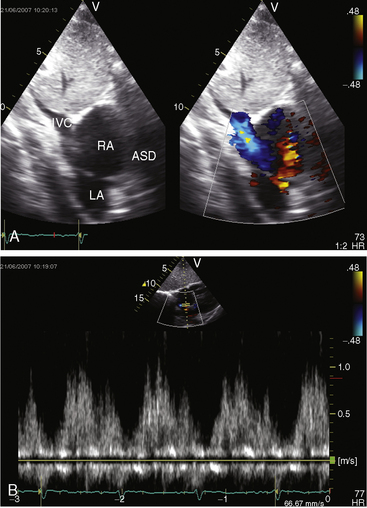
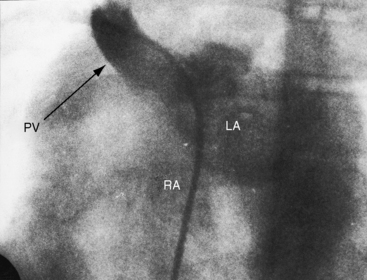
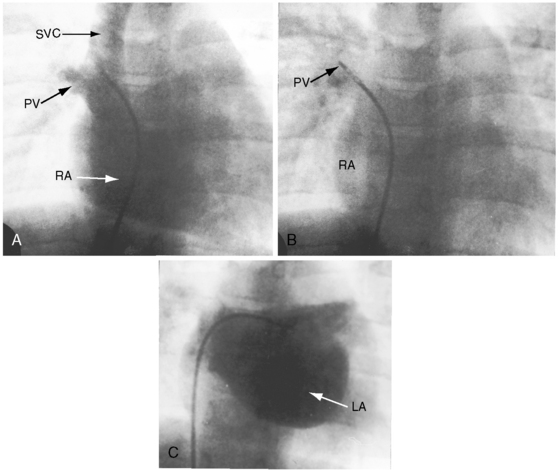
Superior vena caval sinus venosus defects are located immediately below the junction of the superior cava and the right atrium (see Figures 15-2 and 15-48) and vary from small to nonrestrictive. The orifice of the superior vena cava may override the defect, which is therefore biatrial.21 Inferior vena caval sinus venosus defects are located below the foramen ovale and merge with the floor of the inferior cava (see Figures 15-2 and 15-48).15,22 As the valve of the inferior vena cava resorbs, its rudiment becomes the fetal eustachian valve that directs inferior caval blood across the foramen ovale. Persistence of a large eustachian valve (Figure 15-4 and Videos 15-1A and 15-1B) channels inferior vena caval blood across an ostium secundum atrial septal defect (Figure 15-5 and Video 15-2) or across an inferior vena caval sinus venosus defect (see Figure 15-48).22,23 Atrial septal defects are usually located in only one of the foregoing locations, but separate ostium secundum, sinus venosus, and ostium primum defects occasionally coexist.24
Coronary sinus atrial septal defects are uncommon but not rare. As the name implies, the defect is located at the site normally occupied by the right atrial ostium of the coronary sinus (see Figure 15-2)25 and is characterized by an opening in the wall of the distal end of the sinus or by unroofing caused by absence of the partition between the coronary sinus and left atrium. A left superior vena cava inserts into the upper left corner of the left atrium. A relatively rare combination consists of absence of the coronary sinus, a defect in the atrial septum in the location of the ostium of the coronary sinus, and a left superior vena cava connected to the left atrium.25 This combination is necessarily cyanotic because blood from the left superior vena caval enters the left atrium directly.
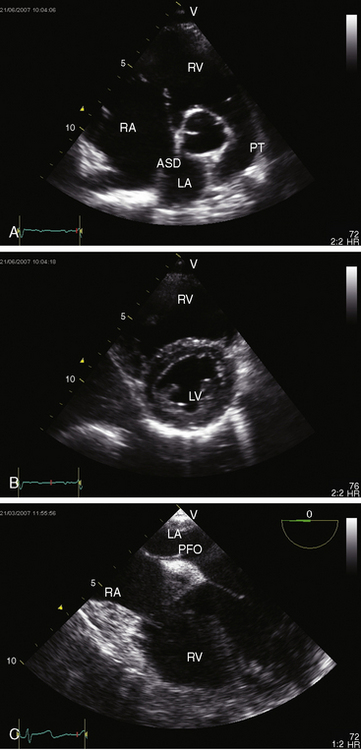
Spontaneous closure of an ostium secundum atrial septal defect refers to sealing of a true tissue defect, and not to cessation of a left-to-right shunt through a valve-incompetent foramen ovale.26,27 Ostium secundum atrial septal defects are seldom symptomatic in infants and young children (see Figure 15-46B and Videos15-3A through 15-3D); but when they are so manifest, approximately one third close spontaneously between 1 and 2 years of age.27 The mechanisms responsible for spontaneous closure remain to be established, but multiple small interatrial septal openings (diameters less than 5 mm) in newborns have a strong tendency to close during the first year of life.18
Anatomic connections and physiologic drainage of pulmonary veins are important distinctions in atrial septal defects. Connection refers to a pulmonary vein that is anatomically contiguous—connected—with a morphologic left atrium or a morphologic right atrium.28,29 Drainage refers to the physiologic pathway of blood from pulmonary veins into the left or right atrium. Pulmonary veins that connect normally can drain anomalously, but pulmonary veins that connect anomalously drain anomalously. Normal right pulmonary veins connect to the left atrium close to the rim of ostium secundum atrial septal defects,29,30 so a substantial portion of right pulmonary venous blood preferentially drains into the right atrium even though the veins connect anatomically to the left atrium (Figure 15-6). Partial anomalous pulmonary venous connection refers to one or more but not all pulmonary veins that connect anomalously to the right atrium.28,31 Total anomalous pulmonary venous connection exists when all four pulmonary veins connect anomalously to the right atrium, directly or indirectly. Ten percent to 15% of ostium secundum atrial septal defects are associated with partial anomalous pulmonary venous connections. Eighty percent to 90% of superior vena caval sinus venosus defects are associated with anomalous connection of the right superior pulmonary vein to the right atrium or superior vena cava (Figures 15-2 and 15-7).21 About 90% of partial anomalous pulmonary venous connections join the right upper or middle lobe pulmonary veins into the right atrium or superior vena cava.28,32 Partial anomalous connection of right pulmonary veins is usually associated with ostium secundum atrial septal defects,33 exceptionally is associated with an intact atrial septum, and may go unrecognized when associated with a restrictive sinus venosus defect (see Figure 15-7). Anomalous connection of left pulmonary veins is far less prevalent (incidence rate about 10%) than anomalous connection of right pulmonary veins and is represented by anomalous connection to the innominate vein or to a persistent left superior vena cava that attaches to the innominate vein. Bilateral partial anomalous pulmonary venous connections are rare.
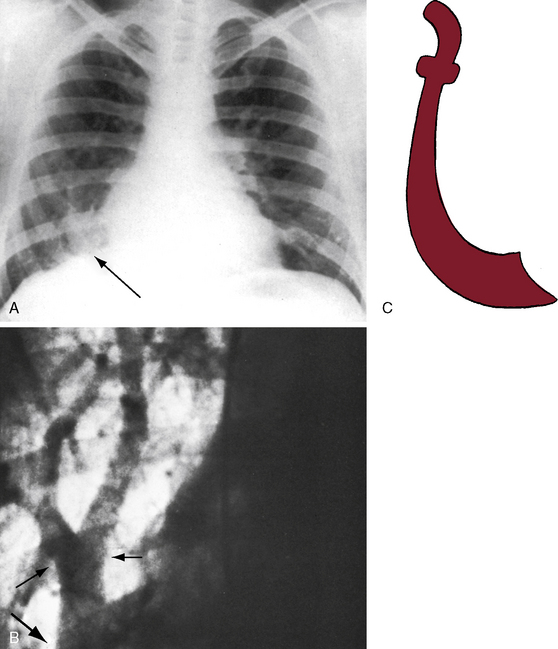
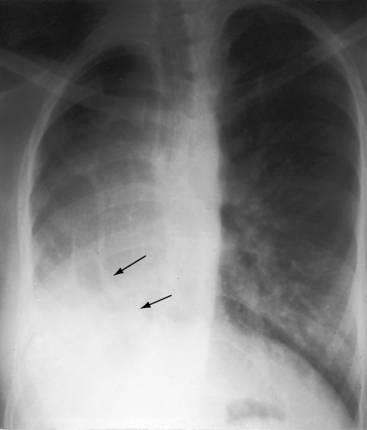
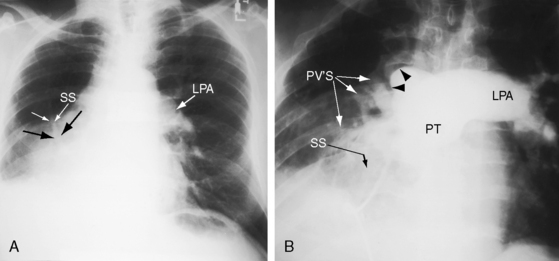
The scimitar syndrome, described in 1836 by Chassinat,34 is a rare anomaly characterized by connection of all of the right pulmonary veins into the inferior vena cava.35–38 The ipsilateral lung and pulmonary artery are usually hypoplastic (Figures 15-8, 15-9, and 15-10). The syndrome rarely involves the left lung.39 The term scimitar refers to a radiologic shadow that resembles the shape of a Turkish sword (see Figure 15-8C). The lower portion of the right lung is perfused by systemic arteries from the abdominal aorta.36,37
In ostium secundum atrial septal defects, anatomic studies of the mitral, tricuspid, and pulmonary valves have disclosed morphologic and architectural modifications.40 The mitral valve abnormalities consist of thickening and fibrosis of leaflets and chordae tendineae attributed to traumatic cusp movements that result from deformity of the left ventricular cavity. The lesions are thought to be the basis for age-related mitral regurgitation.41,42 Superior systolic displacement of the mitral leaflets (mitral valve prolapse) occurs because leaflets with normal area and chordal length are housed in a left ventricular cavity that is reduced in size and abnormal in shape from the leftward position of the ventricular septum (see Figure 15-46B).41
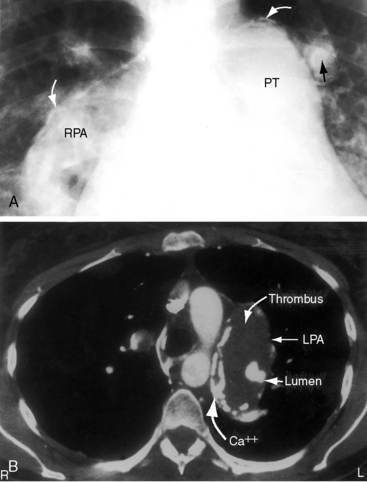
In patients with nonrestrictive atrial septal defects and pulmonary vascular disease, the hypertensive proximal pulmonary arteries dilate aneurysmally and contain mural calcification and intraluminal thrombi that can be massive and occlusive (Figure 15-11).43 Aneurysmal proximal pulmonary arteries may rupture.44 Abnormalities of medial smooth muscle, elastin, collagen, and ground substance reside in the walls of these pulmonary arteries and are held responsible for dilation that is out of proportion to hemodynamic or morphogenetic expectation.44
The physiologic consequences of atrial septal defects depend on the magnitude and chronicity of the left-to-right shunt and on the behavior of the pulmonary vascular bed. When the defect is restrictive, size per se determines the magnitude of the shunt.45 When the defect is nonrestrictive, there is no pressure difference between the right and left atrium, so shunt volume is determined by the relative compliance of the two ventricles.46 During diastole, all four cardiac chambers are in common communication, so blood can flow from the left atrium through the atrial septal defect into the right atrium and across the tricuspid valve into the right ventricle or can flow directly into the left ventricle across the mitral valve. Alternatively, blood from the right atrium can flow across the atrial septal defect into the left atrium across the mitral valve into the left ventricle or directly into the right ventricle across the tricuspid valve. In an ostium secundum atrial septal defect, the right ventricle is thinner and more compliant than the left ventricle, so blood flow is from left atrium through the atrial septal defect across the tricuspid valve into the relatively compliant right ventricle, which thus establishes a left-to-right shunt.46 The shunt reaches its peak in late systole and early diastole; it diminishes throughout diastole; and in late diastole, it is supplemented by atrial contraction (see Figure 15-5B).47,48 A small transient right-to-left shunt coincides with the onset of ventricular systole (see Figure 15-5B). Clinical and experimental studies of instantaneous flow across atrial septal defects have confirmed these flow patterns.47
The fetal circulation is not altered by an atrial septal defect because in utero interatrial flow is normally from right to left through a patent foramen ovale (see Figure 15-46C). At birth, there is little or no shunt in either direction across an atrial septal defect because the compliance of the right and left ventricles is virtually identical.20,49,50 The right ventricle gradually becomes thinner and more compliant than the left ventricle in response to the fall in neonatal pulmonary vascular resistance, so left atrial blood then flows across the atrial septal defect into the more compliant right ventricle.51 Pulmonary blood flow that is received by the right pulmonary veins is channeled into the right atrium because of proximity of the right pulmonary veins to the rim of the atrial septal defect (see previous; see Figure 15-6). Pulmonary blood flow received by the left pulmonary veins is channeled directly into the left atrium and is then shunted across the atrial septal defect. Accordingly, the right ventricle is volume overloaded and the left ventricle is volume underloaded.
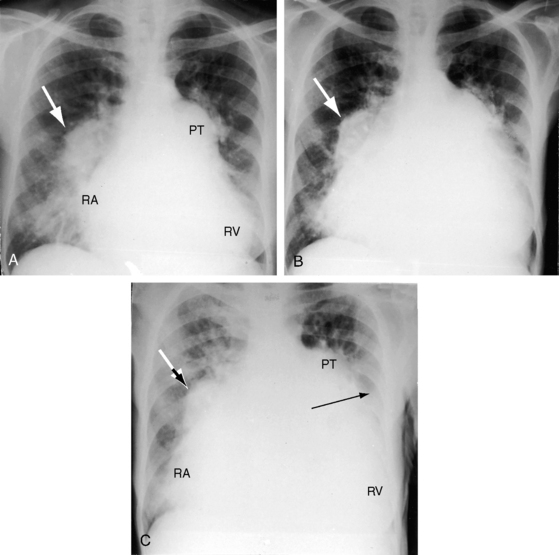
The mature right ventricle is a compliant chamber that readily adapts to volume overload and ejects its increased stroke volume into the low-resistance pulmonary vascular bed.51 Right ventricular function is usually maintained through the fourth decade.51 Ischemic heart disease and systemic hypertension conspire to reduce left ventricular compliance and thus to increase the left-to-right shunt. The additional volume overload of the right atrium provokes atrial fibrillation and atrial flutter, which further increase the left-to-right shunt and result in heart failure (Figure 15-12).
Left ventricular end-diastolic volume, stroke volume, ejection fraction, and cardiac output are decreased in infants and adults with an atrial septal defect,52–54 and ejection fraction tends to fall with exercise.52 Diminished left ventricular functional reserve is related to the mechanical effects of right ventricular volume overload, which displaces the ventricular septum into the left ventricular cavity, reducing its size and changing its shape from ovoid to crescentic (see previous; see Figure 15-46B).42,52,53 In addition, coronary reserve is compromised in the volume-overloaded right ventricle if the left main coronary artery is compressed by a dilated pulmonary trunk.55
An important and poorly understood deviation from the prevailing pattern of an asymptomatic onset of the left-to-right shunt across an atrial septal defect is the occasional infant with development of a large shunt and right ventricular failure.27,56 A left-to-right shunt that begins before the increase in right ventricular compliance has been attributed to more complete emptying of the right ventricle (reduced resistance to discharge). Right ventricular failure ensues because the neonatal right ventricle is volume overloaded before involution of its free wall thickness.57 Although right ventricular failure is occasionally intractable, there is a propensity for clinical improvement because of spontaneous closure of the atrial septal defect.18,27
The paucity of pulmonary vascular disease in patients with nonrestrictive atrial septal defects has been ascribed to the onset of the left-to-right shunt after pulmonary arterial pressure and pulmonary vascular resistance have normalized. A low-resistance low-pressure pulmonary vascular bed accommodates an appreciable increment in blood flow without a rise in pressure.58,59 An exception is the propensity for pulmonary hypertension in patients with atrial septal defects who are born at high altitude.60,61 Pulmonary vascular disease with a right-to-left shunt at sea level occurs in less than 10% of patients with an atrial septal defect and is believed to represent the coincidence in young females of primary pulmonary hypertension and an ostium secundum atrial septal defect (Figure 15-13; see Chapter 14).
Increased resistance to right ventricular discharge can also result from massive occlusive thrombus in dilated hypertensive proximal pulmonary arteries (see previous; see Figures 15-11B and 15-42). Older adults experience a moderate rise in pulmonary artery pressure with persistence of the left-to-right shunt. Thus, pulmonary hypertension with a nonrestrictive atrial septal defect at sea level is bimodal and is represented in young females with coexisting primary pulmonary hypertension or in older adults, male or female, who have moderate pulmonary hypertension with a persistent left-to-right shunt.
The physiologic consequences of an atrial septal defect with partial anomalous pulmonary venous connection are similar if not identical to those of an isolated atrial septal defect with an equivalent net shunt because the hemodynamic fault remains the left-to-right shunt at atrial level.21,62 However, flow through anomalous pulmonary veins into the right atrium is obligatory and is therefore established earlier than shunt flow across an atrial septal defect. When partial anomalous pulmonary venous connection occurs with an intact atrial septum, flow is increased in the segment of lung with the anomalous pulmonary veins because right atrial pressure is lower than left atrial pressure (intact atrial septum). The pressure gradient across the anomalously draining lung is therefore greater than across the normally draining lung.32,33
Anomalous systemic venous drainage from a normally aligned inferior vena cava results in cyanosis with increased pulmonary blood flow. In an ostium secundum atrial septal defect, small amounts of inferior vena caval blood transiently stream across the defect in early systole, a pattern appropriate for the direction of fetal blood from inferior vena cava across a foramen ovale.63 A large persistent eustachian valve sometimes extends from the orifice of the inferior vena cava to the margin of an ostium secundum atrial septal defect (see Figure 15-4), selectively channeling inferior caval blood into the left atrium and causing cyanosis.22,64 A large eustachian valve in the presence of an inferior vena caval sinus venosus atrial septal defect channels inferior caval blood directly into the left atrium.22
History
The female:male ratio is at least 2:1 in patients with an ostium secundum atrial septal defect,57 and the gender ratio in sinus venosus defects and in ostium primum defects is approximately equal.13 Ostium secundum atrial septal defects are sometimes familial, can recur in a several generations,65,66 and have been found in identical twins.67 Familial scimitar syndrome has been reported.68,69 Autosomal dominant inheritance is a feature of atrial septal defect with the Holt-Oram syndrome (see section Physical Appearance).70 Autosomal dominant inheritance tends to be the mode in inheritance in ostium secundum defects with prolonged atrioventricular conduction.71–73 In some members of a family, the atrial septal defect occurs with PR interval prolongation; other family members have PR prolongation with an intact atrial septum71; and still others experience sudden death. Mutations in the NKX2.5 gene have been associated with familial atrial septal defect and progressive prolongation of atrioventricular conduction.74 Concordant familial segregation of atrial septal defect has been reported with the Axenfeld-Reiger Anomaly (see section Physical Appearance).75
Atrial septal defects may go unrecognized for decades because symptoms are mild or absent and physical signs are subtle.13 The soft pulmonary midsystolic flow murmur in children and young adults is often dismissed as innocent (see Chapter 2). Conversely, an atrial septal defect may first come to light in a routine chest x-ray.76 An important exception is the symptomatic infant with an ostium secundum atrial septal defect (see Figure 15-46B) and congestive heart failure followed by spontaneous closure (see previous).26,27,57
About half of patients with a scimitar syndrome are either asymptomatic or only mildly symptomatic when the diagnosis is made, despite varying degrees of hypoplasia of the right lung (see Figures 15-8, 15-9, and 15-10).36,38 However, a small but important group of patients with scimitar syndrome consists of symptomatic infants with cyanosis and pulmonary hypertension.36 Older children and young adults come to light because an x-ray discloses the scimitar sign and the hypoplastic right lung or because of an atrial tachyarrhythmia, recurrent lower respiratory infections, or a murmur.36,38,77
Paul Wood remarked, “In any series of geriatric necropsies atrial septal defect is always represented.”78 Ostium secundum atrial septal defects are among the most common congenital cardiac malformations in adults and account for 30% to 40% of patients over 40 years of age who have not undergone an operation.13,79–81 Patients often survive to advanced age, but life expectancy is not normal. Three quarters of patients are alive through the third decade, but three quarters are dead by age 50 years and 90% are dead by age 60 years.79 Sporadic survivals have been recorded beyond age 70 years, and rare examples are found of patients in their 80s or 90s (see Figure 15-43B).80–83 An exceptional case was a patient who died 3 months before his 95th birthday (see Figure 15-43A).80 Death is often unrelated to the malformation, but when a relationship exists, cardiac failure is the most common cause.
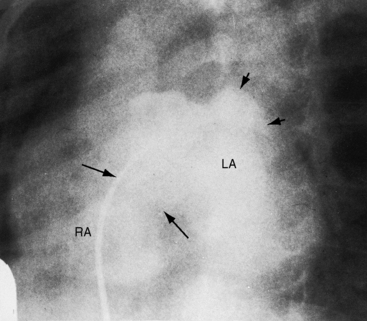
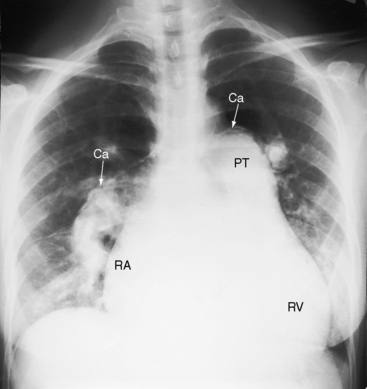
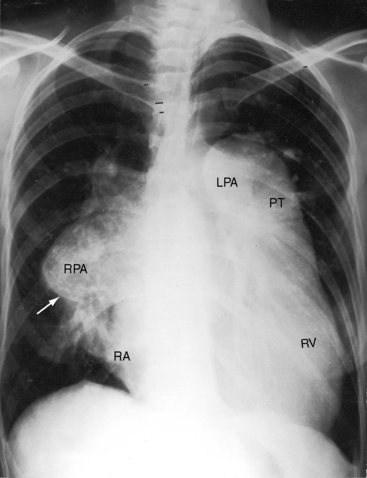
Figure 15-43 A, X-ray from the 95-year-old acyanotic man with a nonrestrictive ostium secundum atrial septal defect. The electrocardiogram (see Figure 15-32) shows atrial fibrillation. Pulmonary arterial and pulmonary venous vascularity are increased. The pulmonary trunk (PT) is dilated, but the ascending aorta is not border-forming. The right atrium (RA) and the right ventricle (RV) are strikingly enlarged. B, X-ray from an 87-year-old acyanotic woman with a nonrestrictive ostium secundum atrial septal defect, severe tricuspid regurgitation, and atrial fibrillation. Pulmonary vascularity is decreased. The pulmonary trunk (PT) is dilated, and the enlarged right branch contains eggshell calcification. The ascending aorta is not border-forming. The right atrium (RA) and right ventricle (RV) are strikingly enlarged. At necropsy, there was a large thrombus in the dilated right pulmonary artery and a smaller thrombus in the dilated left pulmonary artery.
The clinical course of ostium secundum atrial septal defects spans the reproductive years, and most patients are female. It is therefore reassuring that, despite the gestational increase in cardiac output and stroke volume, young gravida with an atrial septal defect generally endure pregnancy, even multiple pregnancies, without tangible ill effects.84 However, brisk hemorrhage during delivery provokes a rise in systemic vascular resistance and a fall in systemic venous return, a combination that augments the left-to-right shunt, sometimes appreciably.84 There is also a peripartum risk of paradoxical embolization from leg veins or pelvic veins because emboli carried by the inferior vena cava traverse the atrial septal defect and enter the systemic circulation.84
Dyspnea and fatigue are early symptoms of an ostium secundum atrial septal defect. The large left-to-right shunt is responsible for a decrease in pulmonary compliance and an increase in the work of breathing. Orthopnea may be experienced because the supine position increases the work of breathing in patients with reduced lung compliance. Platypnea-orthodeoxia is a rare syndrome characterized by orthostatic provocation of a right-to-left shunt across an atrial septal defect or a patent foramen ovale.85,86 Platypnea (dyspnea induced by the upright position and relieved by recumbency) and orthodeoxia (arterial desaturation in the upright position with improvement during recumbency) are features of this rare disorder. Clinical suspicion may originate from the patient who reports that dyspnea is provoked by standing upright.
Recurrent lower respiratory infections are common, especially in children. Although the pulmonary valve is theoretically susceptible to infective endocarditis because of the rapid rate of ejection, only a single case has been reported.87
The conditions of older patients deteriorate chiefly on three counts. First, a decrease in left ventricular distensibility associated with aging, ischemic heart disease, systemic hypertension, or acquired calcific aortic stenosis augments the left-to-right shunt.81,88 Second, an age-related increase in prevalence of paroxysmal atrial tachycardia, atrial fibrillation, and atrial flutter precipitates congestive heart failure (see Figure 15-45).89 Third, mild to moderate pulmonary hypertension in older adults occurs with a persistent left-to-right shunt, so the aging right ventricle is doubly beset by both pressure and volume overload. Pulmonary vascular disease with reversed shunt is believed to represent the coincidence of primary pulmonary hypertension with an ostium secundum atrial septal in young females who are predisposed to both lesions (see Figure 15-13; see previous).59 Importantly, the outlook is better when primary pulmonary hypertension occurs with an atrial septal defect or a patent foramen ovale that permits the right heart to decompress (see Chapter 14).
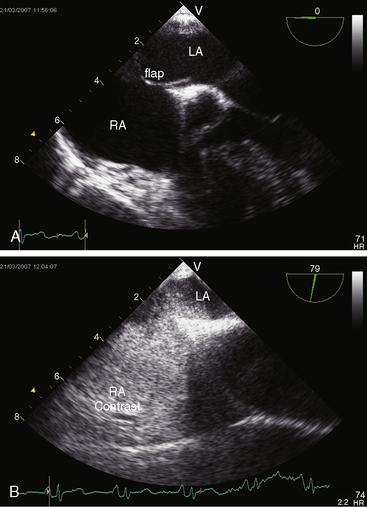
A patent foramen ovale is the most common remnant of the fetal circulation (see Figure 15-46C); it occurs in 10% to 15% of healthy adults and in 20% to 30% of normal hearts at postmortem.10,56,90 The patent foramen varies in anatomic and functional size and is implicated in paradoxical embolization, transient ischemic attacks, venoarterial gas embolism, decompression sickness, and platypnea-orthodeoxia (see previous).56,91
Atrial septal aneurysm is characterized by protrusion beyond the plane of the atrial septum and by rapid, dramatic phasic cardiorespiratory oscillations (see Figure 15-47 and Videos 15-4A through 15-4C).11,12,92 An atrial septal defect may coexist. Cerebral emboli originate from fibrin-platelet aggregates on the left atrial side of the aneurysm and are dislodged by the phasic excursions.92 Atrial septal aneurysms have been incriminated in atrial arrhythmias in children and adults and in the fetus.
Physical Appearance
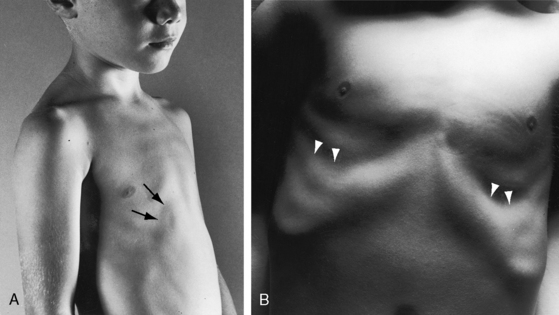
Children with an atrial septal defect may have a delicate gracile habitus, with weight more affected than height (Figure 15-14A), and may have a left precordial bulge with Harrison’s grooves (Figure 15-14B).93 Newborns subsequently found to have an atrial septal defect are on average smaller than their healthy siblings.94 Symptomatic infants may be cyanotic because of the effects of congestive heart failure. Cyanosis also occurs when a large eustachian valve (see previous) selectively channels inferior vena caval blood into the left atrium through an ostium secundum atrial septal defect (see Figure 15-4) or through an inferior vena caval sinus venosus defect (see Figure 15-48).22,63,64
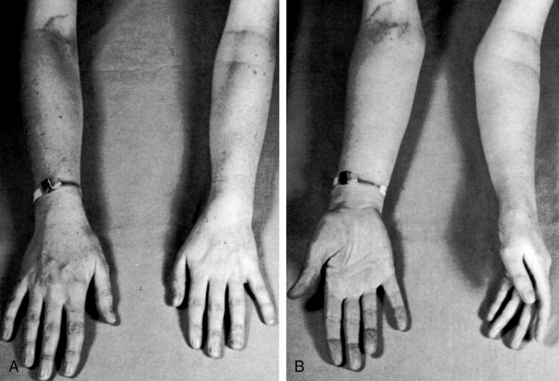
The distinctive physical appearance of the Holt-Oram syndrome heightens suspicion of a coexisting ostium secundum atrial septal defect (Figure 15-15),70,95,96 less commonly of an ostium primum defect. The thumb is hypoplastic with an accessory phalanx that results in triphalangism, a crooked appearance, and difficulty in apposition of thumb to fingertips. The abnormality becomes more obvious when the palms are supinated (see Figure 15-15B). The thumb may be rudimentary or absent, and the metacarpal bone may be small or absent with hypoplasia extending to the radius (Figure 15-16). The bony anomaly ranges from minor changes identified on x-ray to absence of the arm (abrachia) or absent arms with persistent underdeveloped hands (phocomelia).97 Other cardiac malformations occur without prevailing patterns.70 Mutations in a gene on chromosome 12q2 play an important role in skeletal and cardiac development and produce a wide range of partial phenotypes of the Holt-Oram syndrome.98

Patau’s syndrome (trisomy 13) is characterized by polydactyly, flexion deformities of the fingers, palmar crease, microcephaly, holoproscencephaly, cleft lip, cleft palate, and low-set malformed ears. Edward’s syndrome (trisomy 18) is characterized by clenched fists, rocker bottom feet, prominent occiput, low-set malformed ears, and micrognathia (see Figures 19-5 and 20-11). The most common congenital cardiac malformations in trisomy 13 and in trisomy 18 are atrial septal defect, ventricular septal defect, and patent ductus arteriosus.99 An atrial septal defect is associated with the Axenfeld-Rieger anomaly, a genetically heterogeneous autosomal dominant disorder characterized by ocular abnormalities with glaucoma and nonocular abnormalities that include maxillary hypoplasia, dental anomalies, umbilical hernia, and hypospadias.75
Jugular Venous Pulse
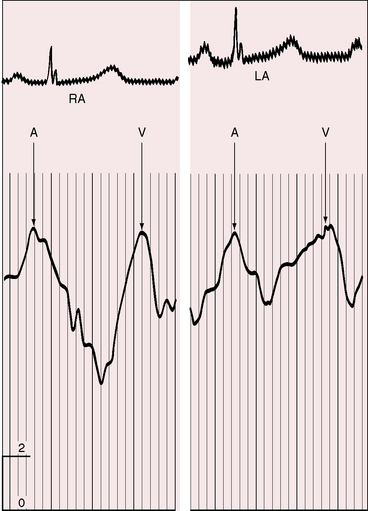
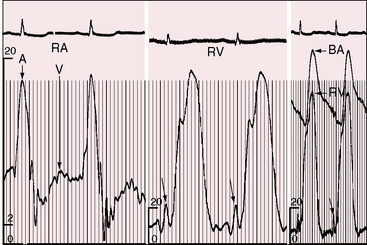
Most important is left atrialization of the jugular venous wave form.100 The crests of the A and V waves tend to be equal as they are in the left atrium (Figure 15-17) because the two atria are in common communication through a nonrestrictive atrial septal defect. The A wave amplitude varies with heart rate as in healthy subjects.101 When left ventricular compliance decreases, left atrial pressure rises, and with it, the right atrial pressure.100,101 Pulmonary vascular disease results in an increased force of right atrial contraction and a dominant, if not giant, A wave (Figure 15-18).
Precordial Movement and Palpation
In 1934, Roesler5 called attention to the conspicuous thrust of the right ventricle in atrial septal defect. The impulse is hyperdynamic but not sustained because the volume-overloaded right ventricle contracts vigorously and empties rapidly into a low-resistance pulmonary vascular bed.102,103 The impulse is especially prominent at the left sternal border during held exhalation and in the subxyphoid area during held inspiration.103 Anterior movement at the left sternal border is accompanied by retraction at the apex because the enlarged right ventricle occupies the apex.6,103 A dilated pulsatile pulmonary trunk is palpable in the second left intercostal space, but a systolic thrill is seldom present despite hyperkinetic right ventricular ejection into a dilated pulmonary trunk.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


