Atrial Septal Defect, Patent Foramen Ovale, and Left Atrial Appendage Closure
Atrial Septal Defect, Patent Foramen Ovale, and Left Atrial Appendage Closure
Philip B. Dattilo MD
Michael S. Kim MD
ATRIAL SEPTAL DEFECTS AND CLOSURE
Atrial Septal Anatomy/Embryology
Septum Primum and Secundum/Foramen Ovale and Fossa Ovalis
The interatrial septum is composed of the septum primum and the septum secundum. In the first developmental stage of the interatrial septum, the septum primum grows from the roof of the atrium toward the endocardial cushions (1, 2), thereby forming the initial separation of the rudimentary right and left atria. As the primum grows, the leading edge is concave (or crescent shaped), resulting in an interatrial communication referred to as the ostium primum, allowing for right-to-left shunting of blood and bypassing of the fetal pulmonary circulation that is obligatory for fetal development. As the ostium primum ultimately closes, fenestrations develop in the superior aspect of the septum and ultimately coalesce to develop into a new interatrial communication referred to as the ostium secundum, allowing for continued right-to-left shunting of blood during fetal gestation.
The septum primum is leftward and posterior to the septum secundum, which is formed by an infolding of the atria directed rightward and anterior to the septum primum. As the septum secundum grows, its leading edge forms the foramen ovale, which lies in continuity with the ostium secundum and allows for continuous right-to-left shunting of blood. As the septum secundum continues to grow, the septum primum continues to thin and regress, ultimately forming a thin flap of tissue covering the left side of the foramen ovale.
With parturition, left atrial pressure exceeds right atrial pressure, thereby forcing the septum primum against the interatrial septum and terminating right-to-left flow through the foramen ovale. Over time, in normal infant development, the foramen ovale fuses, resulting in an intact anatomical structure known as the fossa ovalis. However, in ˜25% of the general population, a small channel—a patent foramen ovale (PFO)—persists (3). The relationship of the septum primum to the secundum results in a flap valve mechanism, wherein the superior and leftward aspect of the septum primum (i.e., the “flap”) can open toward the left atrium in physiologic scenarios where right atrial pressure exceeds that of left atrial pressure (e.g., Valsalva, cough, mechanical ventilation, etc.), allowing for transient right-to-left interatrial shunting and leading to the potential for paradoxical emboli.
Atrial Septal Defect
Secundum Atrial Septal Defect
The most common atrial septal defect (ASD) is a secundum ASD (Fig. 39-1B), accounting for ˜75% of all ASDs (4). The secundumtype defect results from either deficient growth of the septum secundum or excessive resorption of the septum primum (5). Both scenarios result in a centrally located septal defect (near the area of the fossa ovalis in normal hearts) of varying size, shape, and degree of shunting. With the exception of very large secundum ASDs (>35 mm), and those defects with insufficient rim tissue to accommodate a closure device, catheter-based closure techniques are recommended over surgery as first-line therapy for ASD repair/closure.
Primum ASD
Primum ASDs (Fig. 39-1D) (also referred to as Atrioventricular (AV) septal defects, AV canal defects, and endocardial cushion defects) are less common than the secundum type, on the order of 15% to 20% of all ASDs (4). Partial primum ASDs consist of absence of the inferior portion of the interatrial septum and frequently a cleft mitral valve, whereas complete primum ASDs are marked by an inlet ventricular septal defect (VSD) and a single atrioventricular valve (5). The nature and anatomy of primum ASDs are not amenable to catheter-based closure (partly because of their spatial relationship to the AV valves), so surgical patch repair is the recommended therapy for such defects.
Sinus Venosus ASD and Unroofed Coronary Sinus
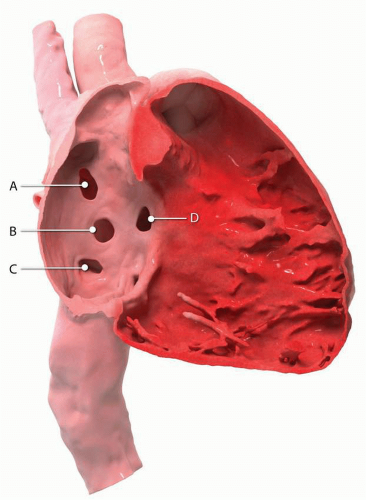
Occurring in significantly lower frequency are sinus venosus (˜5%) and unroofed coronary sinus (<1%) defects. Sinus venosus defects most commonly result from anomalous superior vena cava (SVC) communication with the right atrium (Fig. 39-1A), involving the superior, posterior portion of the septum, and are invariably associated with an anomalous right upper pulmonary vein draining into the right atrium (5). Less frequently, the defect is of the inferior, posterior septum, associated with the inferior vena cava (IVC) and an anomalous right lower pulmonary vein draining into the right atrium (Fig. 39-1C). The unroofed coronary sinus is an open communication between the left atrium and the coronary sinus, allowing for left-to-right shunting through the intact coronary sinus inlet into the right atrium. Neither sinus venosus nor unroofed coronary sinus defects are amenable to catheter-based closure and therefore must be surgically repaired.
FIGURE 39-1 Atrial septal defect morphologies: superior sinus venosus (A), secundum (B), inferior sinus venosus (C), primum (D). (Courtesy of Adam Hansgen)
Indications for ASD Repair/Closure
Recommendations from the ACC/AHA 2008 Guidelines for the Management of Adults with Congenital Heart Disease (4) are listed in Table 39-1.
ASD Closure Devices
Four devices are currently Food and Drug Administration (FDA)approved for the closure of ASDs, of which three are currently available for clinical use: the AmplatzerTM Septal Occluder (St. Jude Medical, St. Paul, MN), AmplatzerTM Multi-Fenestrated (Cribriform) Septal Occluder (St. Jude Medical, St. Paul, MN), Gore® Helex® Occluder (Gore® Medical, Newark, DE) device, and the CardioSEAL STARFlex Septal Occluder (the now defunct NMT Medical Inc., Boston, MA; this device is no longer available).
TABLE 39-1 ACC/AHA Guideline Recommendations for ASD Closure
Recommendation
Class
Level
A sinus venosus, coronary sinus, or primum ASD should be repaired surgically rather than by percutaneous closure.
I
B
Surgeons with training and expertise in CHD should perform operations for various ASD closures. (Level of Evidence: C)
I
C
Surgical closure of secundum ASD is reasonable when concomitant surgical repair/replacement of a tricuspid valve is considered or when the anatomy of the defect precludes the use of a percutaneous device.
IIa
C
Closure of an ASD either percutaneously or surgically is indicated for:
Right atrial and/or right ventricular enlargement, whether or not the patient is symptomatic
I
B
Paradoxical embolism
IIa
C
Orthodeoxia-platypnea
IIa
B
Presence of net left-to-right shunting, pulmonary artery pressure less than two thirds systemic levels, PVR less than two thirds systemic vascular resistance, or when responsive to either pulmonary vasodilator therapy or test occlusion of the defect (patients should be treated in conjunction with providers who have expertise in the management of pulmonary hypertensive syndromes)
IIb
C
Patients with severe irreversible PAH and no evidence of a left-to-right shunt should not undergo ASD closure
III
B
From: Warnes CA, et al. Circulation. 2008;118:2395-2451, with permission.
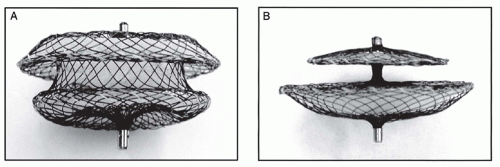
The AmplatzerTM Septal Occluder (ASO) device is approved for the closure of secundum-type ASDs and fenestrated Fontan closures (Fig. 39-2). It is composed of a nitinol (nickel/titanium alloy) mesh with left and right atrial discs and a central waist. The size of the device should match the size of the secundum defect measured with a balloon-sizing technique. In the United States, the ASO comes in sizes ranging from 4 to 38 mm (the diameter of the device waist). The left atrial disc is 12 to 16 mm wider in diameter than the waist (depending on waist size), and 4 mm wider than the right atrial disc. Because of its design, the ASO is considered a “self-centering” device.
The AmplatzerTM Multi-Fenestrated Septal Occluder (aka the Cribriform Occluder) device is approved for closure of multifenestrated secundum-type ASDs. The device is similar in design to the ASO, but differs in that the left and right atrial discs are of the same size with a small central waist. Sizing of the device is according to disc size, and comes in 18-mm, 25-mm, 30-mm, and 35-mm sizes. Like the ASO, the Cribriform occluder is a selfcentering device.
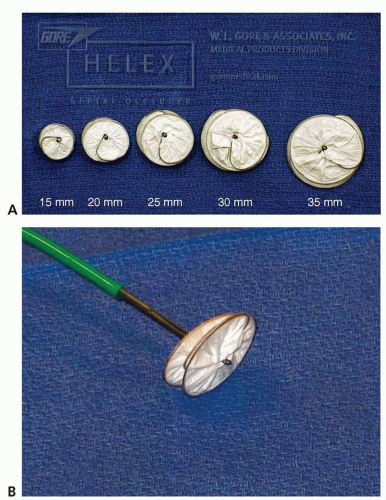
The Gore® Helex® Occluder consists of a nitinol wire frame covered with polytetrafluoroethylene (PTFE) (Fig. 39-3). It is approved for closure of secundum-type ASDs up to 18 mm in diameter and less than 8 mm in thickness. The recommended size of the device is twice the diameter of the defect (2:1 ratio). Available devices sizes are 15 mm, 20 mm, 25 mm, 30 mm, and 35 mm. In contradistinction to the AmplatzerTM devices, the Helex® device will tend to “ride up” and splay against the retroaortic septum secundum (i.e., non-self-centering).
The CardioSEAL device was approved by the FDA for closure of secundum-type ASDs. However, after two negative studies of the related CardioSEAL STARFlex closure device (CLOSURE I [6] and Migraine Intervention with STARFlex Trial [MIST] [7]), the device manufacturer (NMT Medical, Inc.) ceased operations.
Percutaneous Closure Technique
While the specifics of each device’s implantation technique are beyond the scope of this review, there are some important general considerations applying to transcatheter ASD closure that are worth noting.
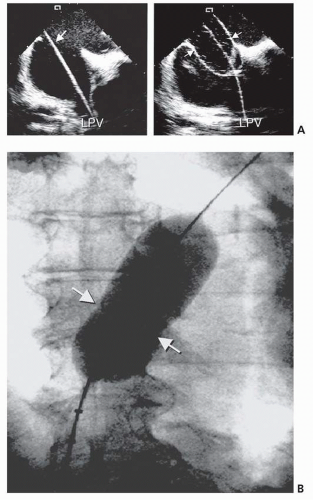
Sizing of the defect is a critical component not only for technical success, but also for minimizing complications while maximizing long-term outcomes. While each device is sized based on its unique design, they all have the capacity to embolize or erode into surrounding structures. As a rule, ASDs should be measured using a compliant sizing balloon, accompanied by invasive (intracardiac or transesophageal) echocardiography (Fig. 39-4). This allows the operator to determine the defect size with a high degree of accuracy. The sizing balloon is advanced across the defect and inflated with low pressure until Doppler color flow across the defect stops. The defect diameter is then measured in its “stretched” form, and an appropriately sized device is selected for closure.
Understanding of the adequacy of the “rim” tissue to allow for device capture is equally important in determining both feasibility of catheter-based closure and ultimate device stability. While retroaortic rim deficiencies are the most common, all rim quadrants of the defect should be carefully examined with echocardiography. In situations where <75% of the defect is accompanied by sufficient rim tissue to safely accommodate a device, surgical defect closure should be strongly considered.
FIGURE 39-2 A: Amplatz Atrial Septal Defect Occluder and B: Cribriform Occluder (also used for Patent Foramen Ovale Occlusion). (From: Alkashkari W, et al. In: Kern MJ, ed. The Interventional Cardiac Catheterization Handbook. Philadelphia, PA: Elsevier pub; 2012, with permission.)
Postclosure Management
Patients are frequently admitted overnight for monitoring, though same day discharge may be considered in certain subsets of patients. Routine care includes postprocedure monitoring of the access site for hematoma formation, complete blood count (CBC) for new onset or worsening anemia, electrocardiograms (ECGs) for signs of pericarditis or arrhythmia, and noninvasive hemodynamics for pericardial effusion.
FIGURE 39-3 A: HELEX® ASD closure devices of various sizes. B: Close-up of attached HELEX® device to delivery cable. (From: Alkashkari W, et al. In: Kern, ed. The Interventional Cardiac Catheterization Handbook. Philadelphia, PA: Elsevier pub; 2012, with permission.)
FIGURE 39-4 Intracardiac echocardiographic images showing defect sizing. A: The exchange wire (arrow) across the defect into the left upper pulmonary vein. Sizing balloon occluding the defect is noted. This is the stretched diameter (arrows in the right) of the defect. B: Cine angiographic image during balloon sizing of the defect, demonstrating the stretched diameter (arrows) of the defect. (From: Alkashkari W, et al. In: Kern, ed. The Interventional Cardiac Catheterization Handbook. Philadelphia, PA: Elsevier pub; 2012, with permission.)
TABLE 39-2 Intention-to-Treat Results of the CLOSURE I Trial
a Defined as stroke or TIA during 2 years of follow-up, death from any cause during the first 30 days, and death from neurologic causes between 31 days and 2 years.
From: Furlan AJ, et al. N Engl J Med. 2012;366:991-999, with permission.
A chest x-ray is recommended within the first 24 hours to check for device positioning and evidence of cardiomegaly suggestive of a large pericardial effusion. More commonly, a transthoracic echo is used to confirm device positioning, rule out pericardial effusion, and ascertain the degree of residual shunt in the first 24 hours, and then at 6 months. It is also typically recommended that patients take aspirin (ASA) 81 to 325 mg daily for the first 6 months, and clopidogrel 75 mg daily for the first 2 to 3 months after device implantation (8
Only gold members can continue reading. Log In or Register to continue