Asthma
GENERAL PRINCIPLES
• Asthma is a disease of the airways characterized by airway inflammation and increased responsiveness (hyperreactivity) to a wide variety of stimuli (triggers).
• Hyperreactivity leads to obstruction of the airways, the severity of which may be widely variable in the same individual.
• As a consequence, patients have paroxysms of cough, dyspnea, chest tightness, and wheezing.
• Other conditions may present with wheezing and must be considered, especially in patients who are unresponsive to therapy, see Table 9-1.
• Asthma is an episodic disease, with acute exacerbations and attacks often interspersed with symptom-free periods.
 Asthma exacerbations occur when airway reactivity is increased and lung function becomes unstable.
Asthma exacerbations occur when airway reactivity is increased and lung function becomes unstable.
 During an exacerbation, attacks occur more easily and are more severe and persistent.
During an exacerbation, attacks occur more easily and are more severe and persistent.
 Asthma attacks are episodes of shortness of breath or wheezing lasting minutes to hours.
Asthma attacks are episodes of shortness of breath or wheezing lasting minutes to hours.
 Patients may be completely symptom-free between attacks.
Patients may be completely symptom-free between attacks.
 Typically, attacks are triggered by acute exposure to irritants (e.g., smoke) or allergens.
Typically, attacks are triggered by acute exposure to irritants (e.g., smoke) or allergens.
 Exacerbations are associated with factors that increase airway hyperreactivity, such as viral infections, allergens, and occupational exposures.
Exacerbations are associated with factors that increase airway hyperreactivity, such as viral infections, allergens, and occupational exposures.
DIAGNOSIS
Clinical Presentation
History
• Acute asthma exacerbation
 Patients with an acute asthma exacerbation present with worsening shortness of breath, wheezing, and/or cough.
Patients with an acute asthma exacerbation present with worsening shortness of breath, wheezing, and/or cough.
 Risk factors for severe exacerbations include
Risk factors for severe exacerbations include
 Previous history of mechanical ventilation
Previous history of mechanical ventilation
 Recurrent need for oral corticosteroids
Recurrent need for oral corticosteroids
 Hospitalization within the past year
Hospitalization within the past year
 Use of more than two canisters per month of inhaled short-acting bronchodilator
Use of more than two canisters per month of inhaled short-acting bronchodilator
 Seizures related to asthma attacks
Seizures related to asthma attacks
• Chronic asthma
 Patients with chronic asthma present with episodic shortness of breath and/or cough, frequently accompanied by wheezing.
Patients with chronic asthma present with episodic shortness of breath and/or cough, frequently accompanied by wheezing.
 Patients often report worsening symptoms with specific exposures (e.g., smoke, volatile cleaning products, gasoline fumes, allergens, dust, etc.).
Patients often report worsening symptoms with specific exposures (e.g., smoke, volatile cleaning products, gasoline fumes, allergens, dust, etc.).
TABLE 9-1 CONDITIONS THAT MAY MIMIC ASTHMA

Physical Examination
• Acute asthma exacerbation
 Initial rapid assessment to identify patients who need immediate intervention is required.
Initial rapid assessment to identify patients who need immediate intervention is required.
 Decreased breath sounds may be noted during severe exacerbations because there is not enough air flow to generate wheeze, thus wheezing is an unreliable indicator of severity of an attack.
Decreased breath sounds may be noted during severe exacerbations because there is not enough air flow to generate wheeze, thus wheezing is an unreliable indicator of severity of an attack.
 Severe airflow obstruction is indicated by:
Severe airflow obstruction is indicated by:
 Pulsus paradoxus >25 mm Hg
Pulsus paradoxus >25 mm Hg
 Accessory respiratory muscle use
Accessory respiratory muscle use
 Nasal alar flaring
Nasal alar flaring
 Inability to speak in full sentences
Inability to speak in full sentences
 Tachycardia >110 beats/min
Tachycardia >110 beats/min
 Tachypnea >28 breaths/min
Tachypnea >28 breaths/min
 Patients with decreased mental status require intubation.
Patients with decreased mental status require intubation.
 SC emphysema should alert the examiner to the presence of a pneumothorax and/or pneumomediastinum.
SC emphysema should alert the examiner to the presence of a pneumothorax and/or pneumomediastinum.
 Impending respiratory muscle fatigue may lead to depressed respiratory effort and paradoxical diaphragmatic movement.
Impending respiratory muscle fatigue may lead to depressed respiratory effort and paradoxical diaphragmatic movement.
 Up to 50% of patients with severe airflow obstruction do not manifest any of the above findings.
Up to 50% of patients with severe airflow obstruction do not manifest any of the above findings.
• Chronic asthma
 Physical examination is frequently normal during symptom-free periods.
Physical examination is frequently normal during symptom-free periods.
 Auscultation of the lungs may reveal wheezing when asthma is symptomatic.
Auscultation of the lungs may reveal wheezing when asthma is symptomatic.
Diagnostic Testing
• Acute asthma exacerbation
 Peak expiratory flow (PEF) assessment:
Peak expiratory flow (PEF) assessment:
 Best method for assessment of severity of asthma attack
Best method for assessment of severity of asthma attack
 Normal values vary with size and age
Normal values vary with size and age
 PEF rate <200 L/min indicates severe obstruction for most adults
PEF rate <200 L/min indicates severe obstruction for most adults
 Serial PEF measurements are effective tools in assessment of patient’s response to therapy
Serial PEF measurements are effective tools in assessment of patient’s response to therapy
 Transcutaneous pulse oximetry:
Transcutaneous pulse oximetry:
 PEF is a poor predictor of hypoxemia and thus transcutaneous pulse oximetry may be necessary
PEF is a poor predictor of hypoxemia and thus transcutaneous pulse oximetry may be necessary
 Supplemental oxygen is administered to maintain oxygen saturations >90%
Supplemental oxygen is administered to maintain oxygen saturations >90%
 Arterial blood gas (ABG):
Arterial blood gas (ABG):
 PEF is a useful screening tool for the presence of hypercapnia
PEF is a useful screening tool for the presence of hypercapnia
 Hypercapnia typically develops when PEF <25% of normal
Hypercapnia typically develops when PEF <25% of normal
 ABG is indicated with PEF remains <25% predicted after initial treatment
ABG is indicated with PEF remains <25% predicted after initial treatment
 Most patients initially have a low PaCO2 secondary to hyperventilation
Most patients initially have a low PaCO2 secondary to hyperventilation
 Normal or elevated PaCO2 indicates inability of the respiratory system to increase ventilation as needed because of severe airway obstruction, increased dead space ventilation, and/or respiratory muscle fatigue
Normal or elevated PaCO2 indicates inability of the respiratory system to increase ventilation as needed because of severe airway obstruction, increased dead space ventilation, and/or respiratory muscle fatigue
 Rising PaCO2 is concerning for impending respiratory failure
Rising PaCO2 is concerning for impending respiratory failure
 Imaging
Imaging
 CXR can be obtained and most frequently reveals hyperinflation.
CXR can be obtained and most frequently reveals hyperinflation.
 Obtaining CXRs in the setting of asthma exacerbation should be limited to patients with suspected complications or significant comorbidities.1
Obtaining CXRs in the setting of asthma exacerbation should be limited to patients with suspected complications or significant comorbidities.1
 Pneumothorax, pneumomediastinum, pneumonia, and atelectasis are sometimes found on CXRs obtained from patients presenting to ER with an asthma exacerbation.
Pneumothorax, pneumomediastinum, pneumonia, and atelectasis are sometimes found on CXRs obtained from patients presenting to ER with an asthma exacerbation.
• Chronic asthma
 Pulmonary function tests (PFTs) are essential for diagnosing asthma.
Pulmonary function tests (PFTs) are essential for diagnosing asthma.
 PFTs demonstrate an obstructive pattern, the hallmark of which is a decrease in expiratory flow rates.
PFTs demonstrate an obstructive pattern, the hallmark of which is a decrease in expiratory flow rates.
 Reduction in the forced expiratory volume over 1 second (FEV1) and a proportionally smaller reduction in the forced vital capacity (FVC), result in a decreased FEV1/FVC ratio (generally <0.70).
Reduction in the forced expiratory volume over 1 second (FEV1) and a proportionally smaller reduction in the forced vital capacity (FVC), result in a decreased FEV1/FVC ratio (generally <0.70).
 With mild obstructive disease that involves only the small airways, the FEV1/FVC ratio may be normal, and the only abnormality may be a decrease in airflow at midlung volumes (forced expiratory flow, 25–75%).
With mild obstructive disease that involves only the small airways, the FEV1/FVC ratio may be normal, and the only abnormality may be a decrease in airflow at midlung volumes (forced expiratory flow, 25–75%).
 Lung hyperinflation causes an increased residual volume and increased residual volume–total lung capacity ratio.
Lung hyperinflation causes an increased residual volume and increased residual volume–total lung capacity ratio.
 The flow–volume loop demonstrates a decreased flow rate for any lung volume and is useful to rule out other causes of dyspnea, such as upper airway obstruction or restrictive lung disease.
The flow–volume loop demonstrates a decreased flow rate for any lung volume and is useful to rule out other causes of dyspnea, such as upper airway obstruction or restrictive lung disease.
 The diagnosis of asthma is supported by an obstructive pattern that improves after bronchodilator therapy, defined as an increase in FEV1 of >12% and 200 mL after 2–4 puffs of a short-acting bronchodilator.
The diagnosis of asthma is supported by an obstructive pattern that improves after bronchodilator therapy, defined as an increase in FEV1 of >12% and 200 mL after 2–4 puffs of a short-acting bronchodilator.
 In patients with chronic, severe asthma with airway remodeling, the airflow obstruction may no longer be completely reversible.
In patients with chronic, severe asthma with airway remodeling, the airflow obstruction may no longer be completely reversible.
 An alternative method of establishing the maximal degree of airway reversibility is to repeat the spirometry after a course of oral corticosteroids (usually prednisone 40 mg/d PO in adults for 10 days).
An alternative method of establishing the maximal degree of airway reversibility is to repeat the spirometry after a course of oral corticosteroids (usually prednisone 40 mg/d PO in adults for 10 days).
 Lack of demonstrable airway obstruction or bronchodilator reversibility does not rule out a diagnosis of asthma.
Lack of demonstrable airway obstruction or bronchodilator reversibility does not rule out a diagnosis of asthma.
 When the spirometry is normal, demonstrating heightened airway responsiveness to a methacholine or exercise bronchoprovocation challenge can substantiate the diagnosis of asthma.
When the spirometry is normal, demonstrating heightened airway responsiveness to a methacholine or exercise bronchoprovocation challenge can substantiate the diagnosis of asthma.
 Imaging: A CXR should be obtained to rule out other causes of dyspnea, cough, or wheezing in patients being evaluated for asthma.
Imaging: A CXR should be obtained to rule out other causes of dyspnea, cough, or wheezing in patients being evaluated for asthma.
TREATMENT
Acute Exacerbations
Indications for hospitalization and level of care:
• Patient response to initial treatment (60–90 minutes after three treatments with short-acting bronchodilator) is a better predictor of need for hospitalization than initial severity of attack.
• Prompt resolution of symptoms and PEF >70% of predicted can be discharged from the ER. Because bronchospasm can recur within 72 hours, education and an asthma action plan are essential.
• Admission to the hospital is recommended when PEF <50% of predicted.
• Recent hospitalization, failure of aggressive outpatient management (using oral corticosteroids), and history of life-threatening exacerbation should all prompt consideration for admission.
• Admission to the ICU should be considered in patients with fatigue, drowsiness, confusion, use of accessory muscles of respiration, hypercapnia, marked hypoxemia, or PEF <150 L/min.
Medications
First Line
• Inhaled short-acting β-adrenergic agonists (SABAs) are the mainstay of bronchodilator therapy. The primary agent is albuterol.
 Albuterol is dosed as 2.5 mg by continuous flow (updraft) nebulization every 20 minutes until improvement or toxicity.
Albuterol is dosed as 2.5 mg by continuous flow (updraft) nebulization every 20 minutes until improvement or toxicity.
 It can also be administered in a metered-dose inhaler (MDI) as 6–12 puffs at similar dosing intervals.
It can also be administered in a metered-dose inhaler (MDI) as 6–12 puffs at similar dosing intervals.
 MDI plus spacer allows lower dose of β-adrenergic agonist to be used and is as effective as nebulized β-adrenergic agonist when performed under direct supervision.
MDI plus spacer allows lower dose of β-adrenergic agonist to be used and is as effective as nebulized β-adrenergic agonist when performed under direct supervision.
• Systemic corticosteroids speed resolution of asthma exacerbations and should be administered to all patients with moderate or severe exacerbations, though the ideal dose is poorly defined.
 Methylprednisolone 40–60 mg IV every 6 hours is the drug of choice for IV therapy.
Methylprednisolone 40–60 mg IV every 6 hours is the drug of choice for IV therapy.
 Oral corticosteroids are as effective if given in equivalent doses (e.g., prednisone 60 mg PO every 6–8 hours).
Oral corticosteroids are as effective if given in equivalent doses (e.g., prednisone 60 mg PO every 6–8 hours).
 Tapering should not begin until there is objective evidence of clinical improvement, generally 36–48 hours.
Tapering should not begin until there is objective evidence of clinical improvement, generally 36–48 hours.
 Patients initially on IV therapy should be switched to PO.
Patients initially on IV therapy should be switched to PO.
 7–14-day tapering dosage of prednisone is usually prescribed in combination with an inhaled corticosteroid (ICS) to be instituted at the beginning of the tapering schedule.
7–14-day tapering dosage of prednisone is usually prescribed in combination with an inhaled corticosteroid (ICS) to be instituted at the beginning of the tapering schedule.
Second Line
• Inhaled anticholinergic medications like ipratropium can sometimes be used in treatment.
 Ipratropium is dosed as 0.5 mg by continuous flow (updraft) nebulization every 2 hours in combination with β-agonist until improvement
Ipratropium is dosed as 0.5 mg by continuous flow (updraft) nebulization every 2 hours in combination with β-agonist until improvement
 Special circumstances in which parasympatholytic therapy may be of benefit:
Special circumstances in which parasympatholytic therapy may be of benefit:
 COPD with asthmatic component
COPD with asthmatic component
 Patients with asthma triggered by ingestions of β-blocker
Patients with asthma triggered by ingestions of β-blocker
 Patients on monoamine oxidase inhibitor (MAOI) therapy at risk for sympathomimetic toxicity secondary to impaired drug metabolism
Patients on monoamine oxidase inhibitor (MAOI) therapy at risk for sympathomimetic toxicity secondary to impaired drug metabolism
• Methylxanthines including theophylline or aminophylline can be used, however with caution.
 IV theophylline or aminophylline in combination with β-agonist results in no further bronchodilation than β-agonist alone.
IV theophylline or aminophylline in combination with β-agonist results in no further bronchodilation than β-agonist alone.
 Toxicity is increased with no benefit.
Toxicity is increased with no benefit.
 Routine use of methylxanthines in the management of acute asthma attacks is not recommended.
Routine use of methylxanthines in the management of acute asthma attacks is not recommended.
• Magnesium sulfate can be considered in severe exacerbations (FEV1 or PEF <40% predicted) that fail to respond to initial treatment with β-agonists and may reduce hospital admission and improve lung function.2
 Magnesium sulfate is dosed as 2 g IV infused over 20 minutes and can be considered in severe exacerbations.
Magnesium sulfate is dosed as 2 g IV infused over 20 minutes and can be considered in severe exacerbations.
 This medication can also be considered in patients with toxicity-limiting β–adrenergic agonist therapy or respiratory failure.
This medication can also be considered in patients with toxicity-limiting β–adrenergic agonist therapy or respiratory failure.
• Epinephrine may rarely be needed for the treatment of asthma and can be administered as aqueous epinephrine 0.3 mL of 1:1000 solution subcutaneously every 20 minutes for up to 3 doses.
 ECG monitoring is necessary
ECG monitoring is necessary
 Should be avoided in patients with known or suspected coronary artery disease
Should be avoided in patients with known or suspected coronary artery disease
• Heliox is a blend of helium and oxygen with a lower density than air. Heliox (70:30 or 80:20 helium:oxygen mixture) can be considered in patients with severe exacerbation (FEV1 or PEF <40% predicted) who fail initial treatment with inhaled bronchodilators.
 Heliox also appears most promising for patients with respiratory acidosis and short duration of symptoms.
Heliox also appears most promising for patients with respiratory acidosis and short duration of symptoms.
 It may also be helpful in avoiding mechanical ventilation.
It may also be helpful in avoiding mechanical ventilation.
• Antibiotics have been shown to be of no benefit when administered routinely for acute asthma exacerbations and are only recommended if indicated for treatment of comorbid conditions (e.g., pneumonia or bacterial sinusitis).
Other Nonpharmacologic Therapies
• Mechanical ventilation is considered in any patient with asthma admitted to the ICU as there is a relatively high morbidity and mortality among asthma patients undergoing invasive mechanical ventilation.3
• Noninvasive positive-pressure ventilation (NIPPV)
 Improves alveolar ventilation and decreases work of breathing.
Improves alveolar ventilation and decreases work of breathing.
 Has been shown to reduce the need for intubation in a selected group of patients with severe asthma.4
Has been shown to reduce the need for intubation in a selected group of patients with severe asthma.4
 NIPPV should only be performed in an ICU setting by physicians with experience in noninvasive ventilation.
NIPPV should only be performed in an ICU setting by physicians with experience in noninvasive ventilation.
 Heliox may be used in conjunction with NIPPV to further assist avoiding invasive ventilation.
Heliox may be used in conjunction with NIPPV to further assist avoiding invasive ventilation.
• Invasive positive-pressure ventilation
 Hyperinflation may result secondary to incomplete expiration of the machine-delivered tidal volumes resulting in intrinsic positive end-expiratory pressure (PEEP), also referred to as auto-PEEP.5
Hyperinflation may result secondary to incomplete expiration of the machine-delivered tidal volumes resulting in intrinsic positive end-expiratory pressure (PEEP), also referred to as auto-PEEP.5
 PEEP may impede venous return leading to decreased cardiac output and hypotension.
PEEP may impede venous return leading to decreased cardiac output and hypotension.
 Strategies to minimize intrinsic PEEP, hemodynamic instability, and barotrauma include:
Strategies to minimize intrinsic PEEP, hemodynamic instability, and barotrauma include:
 Reduced respiratory rate and tidal volume, which may result in permissive hypercapnia
Reduced respiratory rate and tidal volume, which may result in permissive hypercapnia
 Avoidance of ventilator-applied PEEP
Avoidance of ventilator-applied PEEP
 Increased inspiratory airflow rates to maximize the duration of expiration.
Increased inspiratory airflow rates to maximize the duration of expiration.
Chronic, Daily Asthma Management
• The main goals of daily management are
 Control of symptoms while maintaining normal activity and pulmonary function
Control of symptoms while maintaining normal activity and pulmonary function
 Prevention of exacerbations
Prevention of exacerbations
 Minimization of medication toxicity
Minimization of medication toxicity
• The successful management requires four main components6:
 Assessing and monitoring severity
Assessing and monitoring severity
 Patient education
Patient education
 Control of triggers
Control of triggers
 Medication plan for both daily therapy and exacerbations
Medication plan for both daily therapy and exacerbations
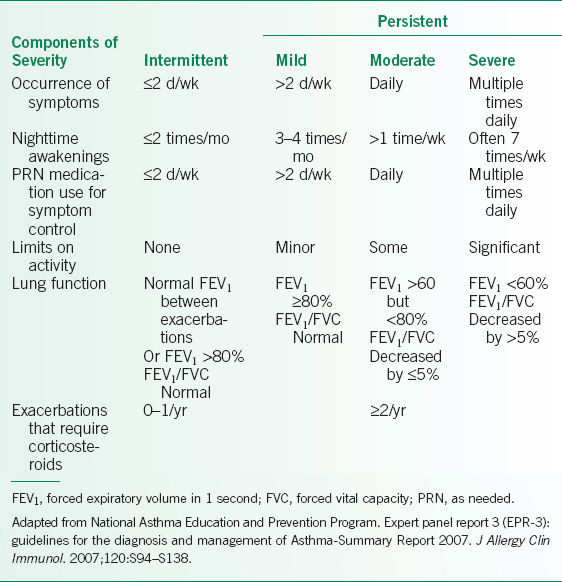
• Asthma severity should be classified as intermittent or mild persistent, moderate persistent, or severe persistent at the first visit, please see Table 9-2.6 If already on treatment, the dose of ICS that provides control can be used to assign severity.
• It is important to assess asthma control at each visit. Standardized questionnaires are available, including:
 Asthma Control Test (ACT)7
Asthma Control Test (ACT)7
 Asthma Control Questionnaire (ACQ)8
Asthma Control Questionnaire (ACQ)8
 Asthma Therapy Assessment Questionnaire (ATAQ)9
Asthma Therapy Assessment Questionnaire (ATAQ)9
• An asthma action plan is a necessary component of the care of the patient with asthma.
 The action plan is a written daily management plan that teaches patients how to avoid factors that aggravate their disease, how to manage daily medications, and how to recognize and deal with acute exacerbations.6
The action plan is a written daily management plan that teaches patients how to avoid factors that aggravate their disease, how to manage daily medications, and how to recognize and deal with acute exacerbations.6
 Patients are taught to avoid exposure to chronic irritants or allergens, specifically those that trigger their disease, including: dust mites, cockroaches, pet dander, viral URI, sinusitis, postnasal drainage, GERD, tobacco and wood smoke, cold air, exercise, aspirin, and NSAIDs.
Patients are taught to avoid exposure to chronic irritants or allergens, specifically those that trigger their disease, including: dust mites, cockroaches, pet dander, viral URI, sinusitis, postnasal drainage, GERD, tobacco and wood smoke, cold air, exercise, aspirin, and NSAIDs.
 PEF provides objective measurement of airflow obstruction.
PEF provides objective measurement of airflow obstruction.
 PEF should be measured early morning before any bronchodilator therapy.
PEF should be measured early morning before any bronchodilator therapy.
 Personal best PEF is identified as highest PEF when disease is under control.
Personal best PEF is identified as highest PEF when disease is under control.
 PEF is then checked with any symptoms or when triggers are identified.
PEF is then checked with any symptoms or when triggers are identified.
 Green zone: 80–100% of best PEF
Green zone: 80–100% of best PEF
 Yellow zone: 50–80% of best PEF
Yellow zone: 50–80% of best PEF
 Red zone: <50% of best PEF
Red zone: <50% of best PEF
 Evidence suggests that an asthma action plan based on symptoms alone is as effective as PEF-based plan.10
Evidence suggests that an asthma action plan based on symptoms alone is as effective as PEF-based plan.10
TABLE 9-2 CLASSIFYING ASTHMA SEVERITY
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


