Data evaluating gender- and age-specific differences in plaque observations on multislice computed tomography (MSCT) are scarce. Accordingly, the aim of this study was to evaluate coronary plaque patterns in men and women in relation to age using MSCT. The findings were compared to observations on grayscale intravascular ultrasound (IVUS) and virtual histology (VH) IVUS. In total, 93 patients (59 men, 34 women) underwent 64-slice MSCT followed by conventional coronary angiography with IVUS. Plaque extent and composition were assessed on MSCT, grayscale IVUS, and VH IVUS. Coronary plaque patterns were compared between men and women in 2 age groups (<65 and ≥65 years old). In patients aged <65 years, more plaques were observed on MSCT in men (6 ± 4 vs 2 ± 2 in women, p <0.001). Also, a larger plaque burden was observed on grayscale IVUS in men (45.7 ± 11.4% vs 36.3 ± 11.6% in women, p <0.001). Similarly, more mixed plaques were observed in men (3 ± 3 vs 1 ± 1 in women, p = 0.003), whereas a larger arc of calcium was detected on grayscale IVUS in men (91.7 ± 93.5° vs 25.7 ± 51.0° in women, p <0.001). On VH IVUS, the prevalence of thin-cap fibroatheroma was higher in men (31% vs 0%) compared to women. In patients aged ≥65 years old, no important differences in plaque patterns were observed between men and women. In conclusion, more extensive atherosclerosis and more calcified lesions were observed in men than in women. These differences were predominantly present in patients aged <65 years and were lost in those aged ≥65 years.
The direct visualization of coronary atherosclerosis rather than testing for obstructive coronary artery disease (CAD) may be more appropriate for the initial assessment of CAD in women. Although plaque burden is traditionally evaluated invasively using intravascular ultrasound (IVUS), noninvasive imaging methods have also become available for this purpose. In previous studies, coronary calcium scoring has been used to evaluate age and gender differences in the extent of coronary calcium. More detailed information, including stenosis severity and plaque composition, can be derived using multislice computed tomography (MSCT). However, data evaluating gender-specific differences in plaque observations on MSCT are scarce. It is important to establish whether these observations hold true for younger and older patients. The purpose of the study was to evaluate gender-specific differences in coronary plaque extent and composition in relation to age using noninvasive MSCT. The findings were compared to invasive coronary plaque observations on grayscale IVUS and virtual histology (VH) IVUS.
Methods
A total of 93 patients were included in the study. All patients presented with chest pain suggestive of CAD. Patients underwent 64-slice multislice computed tomographic coronary angiography, followed within 1 month by conventional coronary angiography in combination with grayscale and VH IVUS of 1 to 3 vessels. The clinical histories of the patients were evaluated before conventional coronary angiography to ensure that neither acute coronary events nor worsening of angina occurred between the examinations. Patients were excluded from the study if contraindications to MSCT were present. IVUS examination was not performed if severe vessel tortuousness, severe luminal narrowing precluding the insertion of the IVUS catheter, or vessel occlusion was present. Informed consent was obtained from all patients, and the study protocol was approved by the local ethics committee.
For comparisons, the patient population was first divided on the basis of gender (men vs women) and second on the basis of age (younger [aged <65 years] vs older [aged ≥65 years] patients).
Multislice computed tomographic coronary angiography was performed using a 64-slice Toshiba Aquilion (Toshiba Medical Systems, Tokyo, Japan) scanner. A helical scan protocol with electrocardiographic gating was applied as described previously. Images were evaluated on a remote workstation with dedicated software (Vitrea 2, Vital Images, Minnetonka, Minnesota; and Advantage, GE Healthcare, Milwaukee, Wisconsin). First, the Agatston coronary calcium score was obtained from the image data set without contrast enhancement. Subsequently, 2 experienced observers evaluated the noninvasive coronary angiograms side by side in consensus. For the assessment of intraobserver variability of plaque assessment in consensus, coronary plaques were repeatedly assessed by 2 observers >6 months later after initial assessment in a subgroup of 20 patients. The presence of coronary plaques was visually assessed as previously described. First, plaques were classified as obstructive or not (≥50% luminal narrowing). Second, the plaques were classified into 3 types: noncalcified (plaques having lower density compared to the contrast-enhanced vessel lumen), calcified (plaques having only high-density structures [≥130 Hounsfield units], without any low-density tissue discernible), and mixed (plaques containing any amount of low-density element with a high-density element embedded in the noncalcified tissue). The images were evaluated on a patient level. The mean numbers of any, nonobstructive, and obstructive plaques were determined per patient. Likewise, the mean numbers of noncalcified, calcified, and mixed plaques were determined.
IVUS examinations were performed with a 20-MHz, 2.9Fr phased-array IVUS catheter (Eagle Eye; Volcano Corporation, Rancho Cordova, California). After the intracoronary administration of nitrates, the catheter was introduced to the distal coronary artery and withdrawn at a continuous speed of 0.5 mm/s to the coronary ostium using an automated pullback device. To define the starting position of the IVUS catheter, cine runs were performed.
To evaluate geometric plaque characteristics, grayscale IVUS data sets were evaluated by an experienced observer, using dedicated software (QCU CMS 4.0; Medis Medical Imaging Systems, Leiden, The Netherlands). Cross-sectional images spaced 0.5 mm apart in the pullback were analyzed within the full length of the examined vessel. The contours of the external elastic membrane (EEM) were identified, and the mean EEM area was calculated per vessel. Subsequently, the lumen-intima interface was identified and mean luminal area was calculated. Plaque area was enclosed by the contours of the EEM and the lumen. Plaque burden was calculated as follows: plaque burden (%) = [Σ(EEM area − lumen area )/ΣEEM area ] × 100. In addition, plaque volume was determined in the 10 mm of the vessel containing the most and least plaque. The percentage of abnormal images (having plaque thickness >0.5 mm) was calculated in each examined vessel. The remodeling index was calculated by dividing the EEM area at the site with most plaque by the EEM area at the proximal reference site. The latter was defined as the frame with largest luminal area located <10 mm from the most diseased frame with no major intervening side branches. Positive remodeling was considered for a remodeling index ≥1.05. Finally, the largest arc of calcium in each examined vessel was obtained.
An experienced observer performed quantitative VH IVUS image analysis on a plaque level using dedicated software (pcVH 2.1; Volcano Corporation). Qualitative VH IVUS analysis was performed side by side in consensus by 2 experienced observers. First, 4 tissues were differentiated and labeled with different colors (fibrotic, fibrofatty tissues, necrotic core, and dense calcium). The mean percentage of each plaque component was obtained in the full length of plaques observed on MSCT. In addition, plaques were visually assessed in 3 consecutive frames <10 mm from the minimal luminal area site and classified into 4 types: (1) pathologic intimal thickening, (2) fibroatheroma, (3) thin-cap fibroatheroma, and (4) fibrocalcific plaque. Plaques were matched between MSCT and VH IVUS as previously described.
First, gender-specific characteristics of coronary atherosclerosis were evaluated in the entire patient population by comparing observations between all men and women. Second, age-related differences between men and women were evaluated. For this purpose, the 2 patient populations (men vs women) were further divided into younger (aged <65 years) and older (aged ≥65 years) patients. Categorical variables were compared between groups using chi-square or Fisher’s exact tests and are expressed as number (percentage). When normally distributed, continuous variables were compared using Student’s t test for independent samples and are expressed as mean ± SD. When not normally distributed, continuous variables were compared using the nonparametric Mann-Whitney test and are expressed as median (interquartile range). All analyses were 2 tailed. To correct for (within) clustering of the variables across the patients, regression analysis was performed for data presented per vessel. For this purpose, a dummy variable was introduced, linking the vessels to different patients. Subsequently, linear regression analysis (if the dependent variable was continuous) or logistic regression analysis (if the dependent variable was categorical) was performed, including gender and the dummy variable as independent variables. The data are presented as correlation coefficients (odds ratios [ORs]) with 95% confidence intervals (CIs). To evaluate the reproducibility of coronary plaque evaluation on MSCT, Cohen’s κ coefficient was calculated. A p value <0.05 was considered statistically significant. Statistical analyses were performed using SPSS version 14.0 (SPSS, Inc., Chicago, Illinois).
Results
Baseline clinical characteristics of the entire patient population are listed in Table 1 . IVUS examinations were available in 208 of 279 vessels (71%) in 93 patients (129 vessels [62%] in men and 79 vessels [38%] in women). VH IVUS examinations were available in a subpopulation of 43 patients (46%) (23 men [54%] and 20 women [46%]). The characteristics of patients with VH IVUS were identical to the general patient population, whereas no differences in CAD risk factors and the use of cardiovascular medication were observed between men and women. In total, 70 vessels were available for VH IVUS analysis (37 vessels [53%] in men and 33 vessels [47%] in women).
| Patient Characteristic | Men | Women | p Value |
|---|---|---|---|
| (n = 59) | (n = 34) | ||
| Age (years) | 61 ± 9 | 64 ± 8 | 0.2 |
| Body mass index (kg/m 2 ) | 27 ± 4 | 26 ± 4 | 0.3 |
| Clinical presentation | |||
| Atypical angina pectoris | 17 (29%) | 13 (38%) | 0.3 |
| Typical angina pectoris | 42 (71%) | 21 (62%) | 0.3 |
| Coronary artery disease risk factors | |||
| Body mass index ≥ 30 kg/m 2 | 18 (31%) | 8 (24%) | 0.6 |
| Hypercholesterolemia ⁎ | 46 (78%) | 26 (77%) | 0.9 |
| Hypertension † | 30 (51%) | 24 (71%) | 0.06 |
| Diabetes mellitus | 11 (19%) | 4 (12%) | 0.4 |
| Smoking | 27 (46%) | 17 (50%) | 0.7 |
| Pretest likelihood ‡ | |||
| Intermediate | 17 (29%) | 17 (50%) | 0.05 |
| High | 42 (71%) | 17 (50%) | 0.05 |
| Previous myocardial infarction | 10 (17%) | 5 (15%) | 0.8 |
| Previous percutaneous coronary intervention | 12 (20%) | 8 (24%) | 0.7 |
| Medications | |||
| Aspirin | 34 (58%) | 21 (62%) | 0.7 |
| Statins | 38 (64%) | 24 (71%) | 0.5 |
⁎ Total cholesterol level ≥5 mmol/L or treatment with lipid-lowering drugs.
† Blood pressure ≥140/90 mm Hg or use of antihypertensive medications.
‡ Determined according to the method of Diamond and Forrester.
Multislice computed tomographic coronary angiograms were of diagnostic quality in all patients. Excellent intraobserver agreement was observed for the detection of any plaque (κ = 1.0), and good intraobserver agreement was observed for the detection of obstructive plaques (κ = 0.80). Coronary plaques were more prevalent in men (6.7 ± 3.8 vs 4.0 ± 3.0 in women, p = 0.001). This observation was related to a higher prevalence of obstructive plaques (2.0 ± 2.2 in men vs 0.7 ± 1.1 in women, p = 0.002), as well as nonobstructive plaques (4.7 ± 3.1 in men vs 3.4 ± 2.8 in women, p = 0.04).
On grayscale IVUS, a larger plaque burden was observed in men (45.7 ± 11.4% vs 36.3 ± 11.6% in women, correlation coefficient 9.8, 95% CI 6.5 to 13.1, p <0.001). The percentage of IVUS frames with plaque was also higher in men (87.8 ± 19.9% vs 70.2 ± 28.3% in women, correlation coefficient 18.3, 95% CI 11.5 to 25.0, p <0.001). In addition, a trend toward a higher mean remodeling index was observed in men (1.04 ± 0.1 vs 0.99 ± 0.1 in women, correlation coefficient 0.03, 95% CI −0.004 to 0.06, p = 0.08).
With regard to plaque composition on multislice computed tomographic coronary angiography, good intraobserver agreement was observed for the classification of plaque type (κ = 0.92). The median coronary calcium score in men was 256.0 (interquartile range 43.5 to 706.5) compared to 72.0 (interquartile range 2.3 to 155.8) in women (p = 0.003). Similarly, the number of calcified plaques on multislice computed tomographic coronary angiography tended to be higher (2.7 ± 3.5 in men vs 1.7 ± 1.9 in women, p = 0.1). Nevertheless, men had significantly more mixed plaques (2.8 ± 3.1) than women (1.3 ± 1.5) (p = 0.01). Interestingly, the number of noncalcified plaques was identical in men and women (1.3 ± 1.8 vs 1.0 ± 1.3, respectively, p = 0.5).
The arc of coronary calcium on grayscale IVUS was larger in men (94.4 ± 88.5° vs 63.6 ± 68.1° in women, correlation coefficient 33.6, 95% CI 6.8 to 60.4, p = 0.01).
On VH IVUS, the amount of fibrotic tissue was less in the plaques of men (53.6 ± 7.4% vs 57.5 ± 8.0% in women, correlation coefficient −5.2, 95% CI −8.2 to 2.3, p = 0.001). The amount of fibrofatty tissue was larger in the plaques of men (28.5 ± 12.2% vs 25.5 ± 10.4% in women, correlation coefficient 4.9, 95% CI 0.5 to 9.3, p = 0.03). No differences were observed in the amount of necrotic core (11.1 ± 6.2% in men vs 10.7 ± 5.9% in women, correlation coefficient −0.2, 95% CI −2.6 to 2.1, p = 0.8) and dense calcium (6.9 ± 6.3% in men vs 6.3 ± 4.8% in women, correlation coefficient 0.6, 95% CI −1.7 to 2.8, p = 0.6). Likewise, no differences were observed in the prevalence of plaque types: pathologic intimal thickening was observed in 10 plaques (16%) in men and in 9 plaques (18%) in women (OR 1.1, 95% CI 0.4 to 3.3, p = 0.8), fibroatheroma in 27 plaques (42%) in men and 20 plaques (40%) in women (OR 1.0, 95% CI 0.4 to 2.2, p = 0.9), thin-cap fibroatheroma in 13 plaques (20%) in men and 6 plaques (12%) in women (OR 1.0, 95% CI 0.3 to 3.3, p = 0.9), and fibrocalcific plaque in 14 plaques (22%) in men and 15 plaques (30%) in women (OR 1.0, 95% CI 0.4 to 2.6, p = 0.9).
In total, 55 patients (59% of the total population) were aged <65 years (39 men [71%] and 16 women [29%]). The mean age was 56 ± 5 years in men and 57 ± 5 years in women (p = 0.4). No differences in the distribution of CAD risk factors, history of CAD, and use of cardiovascular medication were observed between men and women.
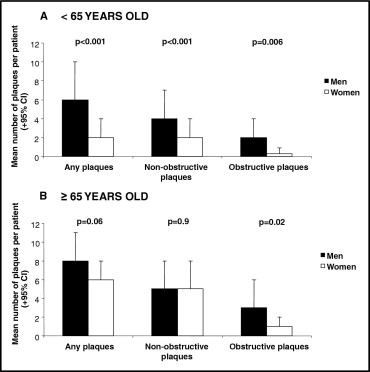
The findings of coronary plaque extent are presented in Figure 1 and listed in Table 2 . On MSCT, the number of coronary plaques was higher in men than in women. The numbers of nonobstructive and obstructive plaques were higher in men ( Figure 1 ). In total, 127 vessels were available for grayscale IVUS analysis (90 vessels in men and 37 vessels in women). Coronary artery diameters were larger in men than in women. In addition, coronary plaque burden was larger in men in the entire vessel as well as in the most and the least diseased coronary artery segments ( Table 2 ).
| Characteristic | Men | Women | Correlation Coefficient (or OR) (95% CI) | p Value ⁎ |
|---|---|---|---|---|
| (n = 90 Vessels) | (n = 37 Vessels) | |||
| Plaque extent and composition on grayscale intravascular ultrasound | ||||
| Vessel length (cm) | 7.0 ± 5.5 | 7.4 ± 3.8 | −0.2 (−2.3 to 1.8) | 0.8 |
| External elastic membrane area (mm 2 ) | 16.2 ± 8.5 | 12.2 ± 3.8 | 3.6 (0.8 to 6.5) | 0.01 |
| Luminal area (mm 2 ) | 8.8 ± 4.5 | 8.9 ± 3.2 | −0.2 (−1.8 to 1.4) | 0.8 |
| Plaque burden (%) | 44.8 ± 12.3 | 27.9 ± 7.9 | 17.2 (12.9 to 21.5) | <0.001 |
| % abnormal frames | 85.9 ± 21.4 | 53.0 ± 26.8 | 32.9 (23.8 to 41.9) | <0.001 |
| Plaque volume in most diseased 10 mm | 100.0 ± 41.9 | 54.9 ± 24.3 | 45.2 (30.4 to 59.9) | <0.001 |
| Plaque volume in least diseased 10 mm | 42.1 ± 29.1 | 18.9 ± 13.2 | 23.5 (13.3 to 33.6) | <0.001 |
| Remodeling index | 1.03 ± 0.1 | 0.99 ± 0.1 | 0.03 (−0.01 to 0.06) | 0.1 |
| Positive remodeling | 27 (31%) | 6 (16%) | 2.1 (0.8 to 5.8) | 0.1 |
| Largest arc of calcium (°) | 91.7 ± 93.5 | 25.7 ± 51.0 | 67.5 (31.9 to 103.0) | <0.001 |
| Plaque composition on virtual histology intravascular ultrasound | ||||
| Lesion length (mm) | 24.6 ± 16.8 | 30.9 ± 17.5 | 0.9 (−12.3 to 11.2) | 0.9 |
| Fibrotic tissue (%) | 51.1 ± 5.1 | 59.1 ± 8.7 | −8.2 (−13.0 to −3.3) | 0.001 |
| Fibrofatty tissue (%) | 27.0 ± 11.5 | 26.7 ± 10.2 | −0.5 (−8.8 to 7.8) | 0.9 |
| Necrotic core (%) | 12.8 ± 6.8 | 8.5 ± 4.1 | 4.2 (−0.3 to 8.8) | 0.06 |
| Dense calcium (%) | 9.1 ± 7.8 | 5.7 ± 3.7 | 4.5 (−0.5 to 9.5) | 0.08 |
| Pathologic intimal thickening | 2 (7%) | 3 (23%) | 0.1 (0.01 to 1.6) | 0.1 |
| Fibroatheroma | 8 (28%) | 5 (39%) | 0.6 (0.1 to 2.7) | 0.5 |
| Thin-cap fibroatheroma | 9 (31%) | 0 (0%) | 0.9 (0.8 to 1.0) | 0.04 |
| Fibrocalcific | 10 (34%) | 5 (38%) | 1.8 (0.4 to 8.8) | 0.4 |
The findings of coronary plaque composition are presented in Figure 2 and listed in Table 2 . The median coronary calcium score on MSCT in men was 216.0 (interquartile range 4.0 to 714.0) compared to 3.5 (interquartile range 0 to 109.0) in women (p = 0.003). A larger number of mixed plaques was observed in men than in women ( Figure 2 ).
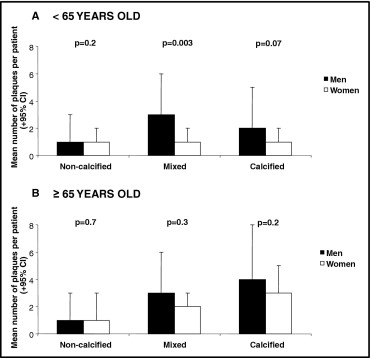
The arc of coronary calcium on grayscale IVUS was larger in men than in women ( Table 2 ). VH IVUS was available in 32 vessels of 21 patients (21 vessels in men and 11 vessels in women). The plaques in women contained more fibrotic tissue, whereas a trend toward more necrotic core was observed in the plaques of men. Thin-cap fibroatheromas were observed exclusively in the plaques of men ( Table 2 ).
In total, 38 patients (41% of the total population) were aged ≥65 years (20 men [53%] and 18 women [47%]). The mean age was 72 ± 4 years in men and 70 ± 4 years in women (p = 0.2). No differences in the distribution of CAD risk factors, history of CAD, and use of cardiovascular medication were observed between men and women.
The findings of coronary plaque extent are presented in Figure 1 and listed in Table 3 . No differences were observed in the prevalence of any and nonobstructive plaques. Nevertheless, obstructive plaques were still more frequently present in men ( Figure 1 ).



