Spasm of the left main coronary artery (LM) is considered to be rare. We investigated the angiographic characteristics of the LM in patients with combined LM and disease involving additional vessels, who underwent coronary artery bypass grafting (CABG) and underwent repeat coronary angiography within 5 years of the CABG, to examine the apparent frequency of spasm of the LM on initial angiography and its possible predictors. A retrospective analysis was performed of patients who underwent coronary angiography in our institute, who were found to have significant LM stenosis and disease involving additional vessels, underwent CABG and repeat coronary angiography within 5 years of the CABG. Data on angiographic characteristics of the LM on the initial angiogram were investigated. Of 84 patients, 17 (20%) were found to have a normal LM on repeat angiography (group A), and 67 (80%) demonstrated significant stenosis (group B). The degree of LM stenosis was milder in the initial angiogram in group A than in group B (64 ± 15% vs 72 ± 14%, p = 0.047). Most patients in group A demonstrated tubular LM stenosis at initial catheterization in comparison to group B (71% vs 18%). Using multivariate analysis, the only predictor for a normal LM at repeat catheterization was found to be tubular stenosis at initial catheterization (odds ratio 123, 95% confidence interval 4.0 to 3696). In conclusion, LM coronary spasm is a common finding, particularly in those with the appearance of tubular stenosis, and it should be excluded even in patients with additional coronary disease in certain instances to prevent unnecessary CABG.
Spasm of the left main coronary artery (LM) is considered to be a rare phenomenon. It should be suspected, particularly in instances of isolated LM disease. We recently described that in patients with isolated LM stenosis referred for coronary computerized tomography angiography, 36% were found to have nonobstructive disease. Patients with LM stenosis and concomitant disease of other coronary arteries are usually referred for revascularization, mainly coronary artery bypass grafting (CABG). In some of these patients, there exists a possibility of LM spasm and not true atherosclerotic disease. This is an important issue, especially in patients without significant disease of the proximal left anterior descending (LAD) artery, in whom coronary revascularization with drug-eluting stents may be the treatment of choice, instead of CABG. We sought to investigate the angiographic characteristics of the LM, in patients with LM combined with disease in other vessels, who underwent CABG and repeat coronary angiography within 5 years of the CABG and were found to have a normal LM on the second angiogram, to elucidate factors reflecting probable spasm of the LM on initial angiography.
Methods
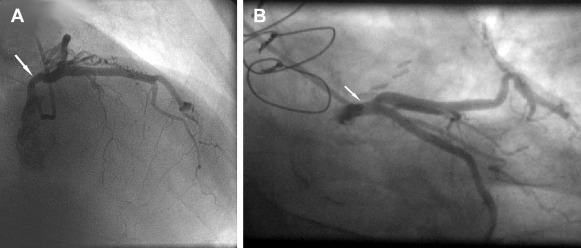
We investigated all patients who underwent coronary angiography in our institute from January 1, 2000, to July 31, 2015, who were found to have significant LM stenosis combined with disease in other vessels and underwent CABG and repeat coronary angiography within 5 years of the CABG. We chose a 5-year cutoff to reduce the possibility of the development of significant new LM stenosis. Patients were divided into 2 groups, those with significant LM stenosis in the repeat catheterization and those with a normal LM, in whom we presumed that the previous stenosis was in fact due to spasm. The demographic and angiographic characteristics (of the LM stenosis on initial angiography) were defined and compared between the groups. Most patients were catheterized using 6Fr left Judkins catheters and a few with 5Fr, the vast majority using the radial technique. Pressure was monitored continuously, and the occurrence of pressure ventricularization was mentioned in the procedure report. In our laboratory, we defined tubular stenosis as a finding of left main diameter smaller than one of its main branches, along most of the length of the LM ( Figure 1 ). The data were obtained from an electronic database of the catheterization laboratory. All angiograms were reviewed by an experienced angiographer (RI). The initial angiogram was reviewed blinded to the results of the second. In our laboratory, the degree of stenosis is estimated visually.
Independent 2-tailed Student t test was used to compare continuous variables. Chi-square test or Fisher’s exact test was used to compare categorical variables. Angiographic variables associated with the absence of LM disease on the second angiography were identified initially using a univariate analysis. Subsequently, independent predictors were identified using an unconditional multivariate logistic regression model and were expressed as odds ratios (ORs) with their corresponding 95% confidence interval (CI). Angiographic variables with a p value <0.1 in the univariate analysis or those selected by a clinical judgment were included in the model. The 2-sided level of significance was set at 0.05. Data were analyzed using the SPSS statistical software package (SPSS Inc., Chicago, Illinois).
Results
Of 37,960 patients who underwent coronary angiography in our institute from January 1, 2000, to July 31, 2015, 84 with significant LM stenosis combined with disease in other vessels underwent CABG and had a repeat coronary angiography within 5 years of the initial angiography. Of these 84 patients, 17 (20%) were found to have a normal LM on repeat angiography (group A) and 67 (80%) demonstrated significant stenosis (group B).
Demographic, clinical, and angiographic findings are presented in Table 1 . There were no differences between groups regarding demographic characteristics. The interval between the 2 angiographic studies was significantly longer in group A than in group B.
| Variable | Left Main Narrowed on Second Angiography | P value | ||
|---|---|---|---|---|
| No (n=17) | Yes (n=67) | |||
| Age (years) | 64.7 ± 9.6 | 63.8 ± 9.7 | 0.71 | |
| Women | 9 (53%) | 45 (67%) | 0.27 | |
| Diabetes Mellitus | 8 (47%) | 26 (39%) | 0.54 | |
| Hypertension | 8 (47%) | 46 (68%) | 0.09 | |
| Smokers | 7 (41%) | 29 (43%) | 0.87 | |
| Interval between angiograms (months) | 28 ± 19 | 19 ± 15 | 0.04 | |
| LM 1 st angio- % of stenosis | 64 ± 15 | 72 ± 14 | 0.047 | |
| Site of LM stenosis in first angio | Ostial | 4 (24%) | 17 (25%) | <0.001 |
| Body | 0 (0%) | 2 (3%) | ||
| Bifurcation | 1 (6%) | 36 (54%) | ||
| Tubular | 12 (71%) | 12 (18%) | ||
| Pressure ventricularization | 2 (12%) | 10 (15%) | 1 | |
| Calcification of LM in first angio | 3 (18%) | 22 (33%) | 0.22 | |
| Diameter of LM in first angio (mm.) | 3.0 ± 0.8 | 3.6 ± 0.9 | 0.007 | |
| Number of diseased vessels in first angio | 2.4 ± 0.8 | 2.3 ± 0.9 | 0.68 | |
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


