Anatomy of the Esophagus
Victor Maevsky
Thomas J. Watson
Anatomy of the Esophagus
Overview
The esophagus is a muscular tube extending from the pharynx to the stomach and bordered by two sphincters. It has one primary responsibility: the aboral transport of ingested food, liquid, and saliva. Prevention of reflux of gastric contents is inherent to this task. Unlike other portions of the gastrointestinal tract, the esophagus has no known endocrine, exocrine, immunologic, digestive, absorptive, or secretory role.
The esophagus starts as a continuation of the pharynx, is normally 20 to 30 cm in length in adults, and terminates at the cardia of the stomach. With the head in its normal anatomic position and the neck in neutral flexion, the transition from pharynx to esophagus begins at the inferior edge of the cricoid cartilage opposite the lower border of the sixth cervical vertebra (Fig. 129-1). The esophagus descends along the front of the vertebral column, through the superior and posterior mediastinum; it then passes through the diaphragm and enters the abdomen, ending at the gastroesophageal junction opposite the 11th thoracic vertebra. The esophagus is normally anchored firmly to the cricoid cartilage at its upper end and to the diaphragm at its lower end. Flexion and extension of the neck or deglutition move these points of fixation craniad the distance of one vertebral body. The general orientation of the esophagus is vertical, with several curves in its course. At its commencement, it is situated in the midline with deviation to the left side as far as the root of the neck. It gradually passes to the midline again at the level of the fifth thoracic vertebra, and finally inclines to the left as it passes forward to the esophageal hiatus in the diaphragm. The esophagus also demonstrates anteroposterior flexures corresponding to the curvatures of the cervical and thoracic portions of the vertebral column.
Radiographic, Endoscopic, and Manometric Anatomy of the Esophagus
Radiographically, the appearance of the esophagus corresponds to its normal anatomy. On the anteroposterior radiograph, the esophagus lies in the midline with a deviation to the left in the lower portion of the neck and upper portion of the thorax. It returns to the midline in the midportion of the thorax near the bifurcation of the trachea (Fig. 129-2A). In the lower portion of the thorax, the esophagus again deviates to the left upon entry into the abdominal cavity through the diaphragm.
On the lateral radiograph, the esophagus follows the posterior curve of the vertebral column except for the lower thoracic portion, where it curves anteriorly to pass through the diaphragmatic hiatus (Fig. 129-2B). This posterior curve and its terminal left anterior deviation are of particular importance in the performance of rigid diagnostic and therapeutic esophagoscopy. During this procedure, the patient’s position should allow full extension of the cervical and thoracic spine so that the rigid scope can be manipulated safely through the terminal arc. As a result of these anatomic configurations, the distal esophagus is the second most common site of iatrogenic esophageal perforation during rigid endoscopy, the first being the narrow entrance of the esophagus at the level of the cricopharyngeus.
Three areas of normal anatomic narrowing in the esophagus are commonly seen during esophagoscopy or contrast esophagogram. The superiormost narrowing is caused by the cricopharyngeus muscle at the anatomic border of the pharynx and proximal esophagus. This narrowest point of the esophagus with an average luminal diameter of 1.5 cm is the most common site of iatrogenic perforation. The crossing of the left mainstem bronchus and the aortic arch results in indentation of the anterior and left lateral esophageal wall, causing the second narrowing of the esophagus, with an average luminal diameter of 1.6 cm. The most inferior narrowing of the esophagus is at the diaphragmatic hiatus and is caused by the physiologic lower esophageal sphincter. There is great variation of the luminal diameter at this point, depending upon the normal distention of the esophagus by the passage of a food bolus, with measurements ranging from 1.6 to 2.5 cm.
The shape of the native, resting esophagus is determined by its contiguous structures as well as by the body cavities it traverses. As assessed by barium esophagography, the cervical esophagus is flattened owing to compression by surrounding structures; the thoracic portion is more rounded because of the negative-pressure environment of the thorax; and the abdominal portion is again flattened owing to positive intra-abdominal pressure. Just above the level of the diaphragm, the esophagus develops a distinct dilatation, perhaps due to outflow resistance imposed by the lower esophageal sphincter as well as a relative lack of buttressing by adjacent organs.
Measurements obtained during endoscopic examination (Fig. 129-3) reveal the average distance from the incisor teeth to the top of the stomach to be 38 to 40 cm in men and 36 to
38 cm in women. These distances are proportionately less in children, being 18 cm at birth, 22 cm at the age of 3 years, and 27 cm at the age of 10. In men, the length of the esophagus from the cricopharyngeus muscle to the gastroesophageal junction ranges from 23 to 30 cm with an average of 25 cm. In women, the range is from 20 to 26 cm with an average of 23 cm. The distance from the incisor teeth to the cricopharyngeus is 15 cm in men and 14 cm women. The bifurcation of the trachea and the indentation of the aortic arch range between 24 and 26 cm from the incisor teeth. When esophageal surgery is being planned, it is helpful to locate intraluminal tumors, strictures, or other pathology in reference to this landmark to help guide a decision regarding a right or left thoracotomy approach and avoid interference with the aortic arch.
38 cm in women. These distances are proportionately less in children, being 18 cm at birth, 22 cm at the age of 3 years, and 27 cm at the age of 10. In men, the length of the esophagus from the cricopharyngeus muscle to the gastroesophageal junction ranges from 23 to 30 cm with an average of 25 cm. In women, the range is from 20 to 26 cm with an average of 23 cm. The distance from the incisor teeth to the cricopharyngeus is 15 cm in men and 14 cm women. The bifurcation of the trachea and the indentation of the aortic arch range between 24 and 26 cm from the incisor teeth. When esophageal surgery is being planned, it is helpful to locate intraluminal tumors, strictures, or other pathology in reference to this landmark to help guide a decision regarding a right or left thoracotomy approach and avoid interference with the aortic arch.
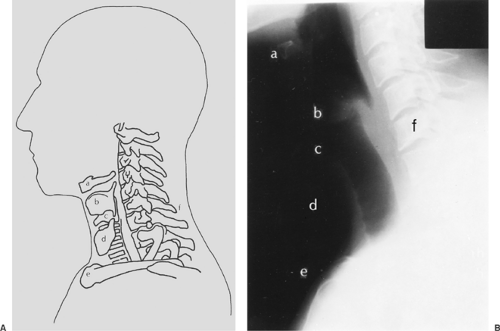 Figure 129-1. A: Topographic relationships of the cervical esophagus: (a) hyoid bone, (b) thyroid cartilage, (c) cricoid cartilage, (d) thyroid gland, (e) sternonclavicular joint, (f) C6. B: Lateral radiographic appearance. |
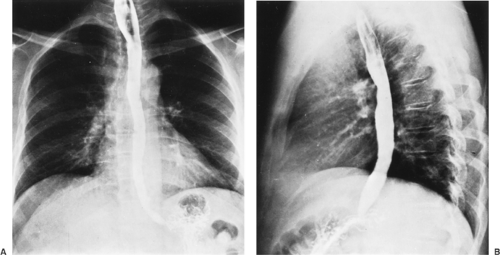 Figure 129-2. Barium esophagogram. A: Anteroposterior view. B: Lateral view. |
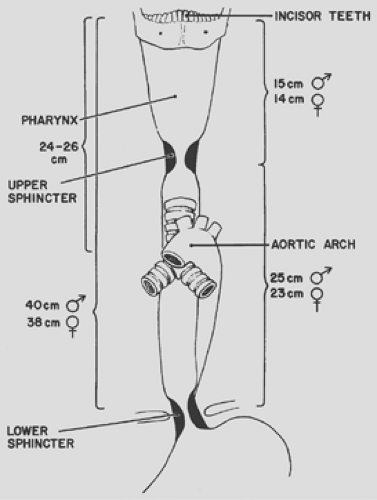 Figure 129-3. Important clinical endoscopic measurements of the esophagus in adults. |
Esophageal length may be determined by manometric assessment. The distance between the bottom of the upper esophageal sphincter and the top of the lower esophageal sphincter represents the length of the esophageal body and varies according to the height of the individual (Fig. 129-4).
Anatomic Relations of the Esophagus
Relationship of the Esophagus to the Hypopharynx
The esophagus serves as a conduit from the pharynx to the stomach. The pharyngeal musculature consists of three overlapping broad, flat, fan-shaped constrictors (Fig. 129-5). The superior constrictor arises mainly from the medial pterygoid plate, the middle constrictor arises from the hyoid bone, and the inferior constrictor arises from the thyroid and cricoid cartilages. These muscles originate bilaterally, joining with their counterparts in the posterior midline to create a median posterior raphe.
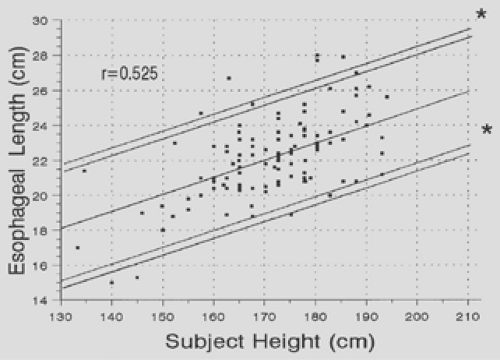 Figure 129-4. Nomogram of subject’s height versus esophageal length. |
The upper orifice to the esophagus is collared by the cricopharyngeus muscle. This muscle originates from both edges of the cricoid cartilage and forms a continuous transverse muscle band without an interruption by a median posterior raphe. The fibers of this muscle blend inseparably with those of the inferior pharyngeal constrictor above and the inner circular muscles of the cervical esophagus below. The cricopharyngeus can be conceptualized as an inferior extension of the inferior constrictor muscle. The inferior constrictor thus has two parts: an upper, or retrothyroid, portion with diagonal fibers, and a lower, or retrocricoid, portion, with transverse fibers. These two parts of the same muscle possess quite distinct functions, the upper portion acting in a propulsive fashion to move a swallowed bolus from the pharynx into the esophagus and the lower portion serving as an upper esophageal sphincter.
Relationship of the Cervical Esophagus to Structures and Fascial Planes of the Neck
The cervical portion of the esophagus is approximately 5 cm long and is situated with the trachea and the main substance of
the thyroid gland in front and the vertebral column and longus colli muscles behind. The esophagus is separated from these structures by loose areolar tissue. On either side, the esophagus is in relation with the common carotid artery sheaths and parts of the thyroid lobes.
the thyroid gland in front and the vertebral column and longus colli muscles behind. The esophagus is separated from these structures by loose areolar tissue. On either side, the esophagus is in relation with the common carotid artery sheaths and parts of the thyroid lobes.
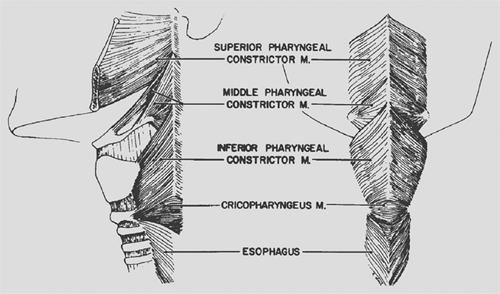 Figure 129-5. External muscles of the pharynx. |
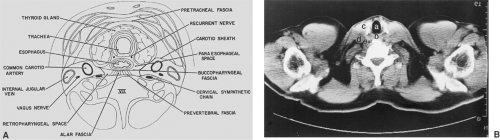 Figure 129-6. A: Cross section of the neck at the level of the thyroid isthmus. B: Computed tomographic appearance viewed from above: (a) trachea, (b) esophagus, (c) left thyroid lobe, (d) internal jugular vein, (e) common carotid artery. |
The esophagus descends between the trachea and the vertebral column from the level of the sixth cervical vertebra posteriorly and the suprasternal notch anteriorly to the level of the interspace between the first and second thoracic vertebrae. The recurrent laryngeal nerves lie in the right and left tracheo- esophageal grooves. Owing to the slight left cervical esophageal deviation, the left recurrent nerve lies closer to the esophagus than the right nerve, which takes a more lateral course around the right subclavian artery.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


