Achalasia and Esophagectomy
Presentation
A 39-year-old Hispanic woman who immigrated to the United States 18 years ago is referred to you with increasing symptoms of dysphagia, which started with solids 2 years ago and now has progressed to liquids. She has lost 30 pounds in the past 8 months. In addition, she is awakened at night by a worrisome choking sensation and coughing spells. Occasionally, she feels that her food backs up into her throat. The patient denies fever, chills, and night sweats. Past medical history is significant for asthma and a bleeding stomach ulcer 5 years ago, for which she underwent a resection. Her physical examination is only remarkable for severe halitosis. Auscultation of the lungs reveals no wheezing or rhonchi. The heart tones are normal, with no murmurs.
Recommendation
Upper gastrointestinal (GI) study.
▪ Upper GI Studies
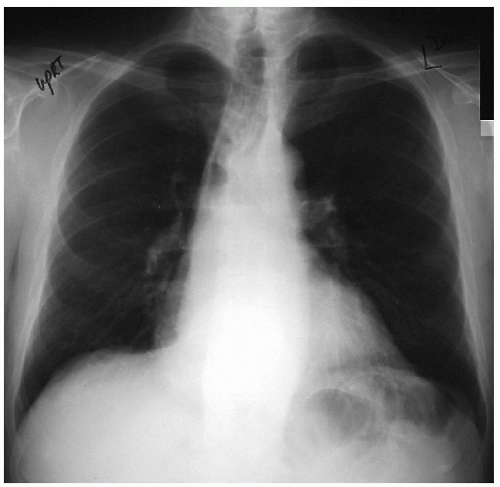
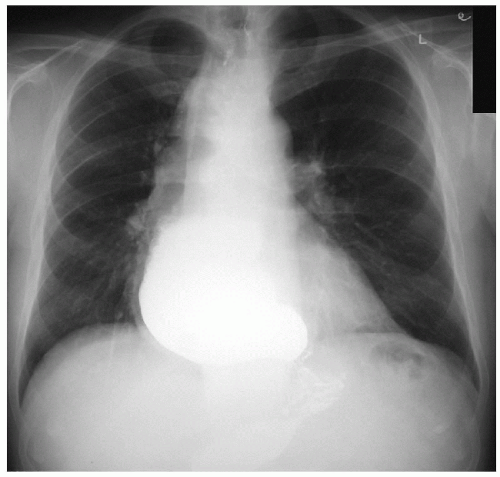 Figure 44-3 |
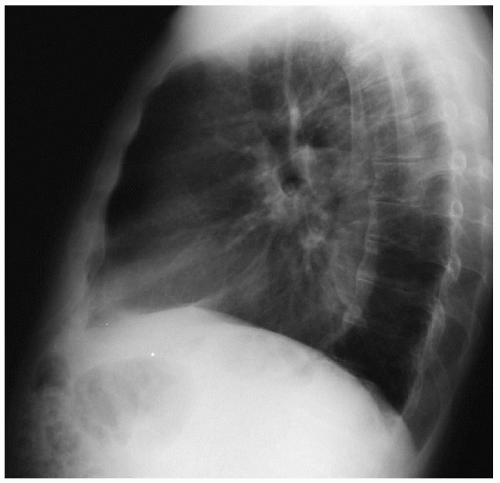
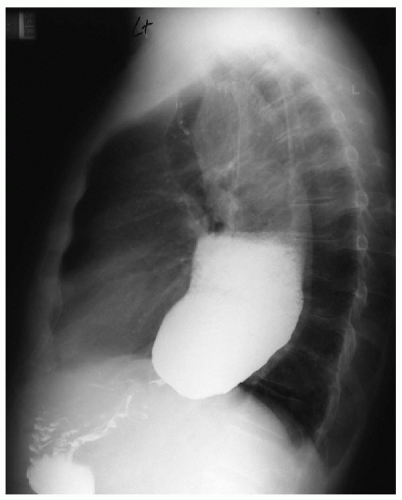 Figure 44-4 |
Upper GI Report
A late-phase contrast esophagram reveals retained contrast with an air-fluid level in a dilated esophagus. Contrast can be seen trickling into the stomach through an obstructed segment. There is some contrast in the small bowel.
Differential Diagnosis
The symptom complex manifested by this patient may be seen with many pathologic conditions of the esophagus, such as carcinoma, stricture, and dysmotility. Motility disorders may be primary or secondary. Some examples of primary disorders include achalasia, diffuse esophageal spasm, or nutcracker esophagus. Secondary disorders include entities such as diabetes mellitus, Chagas’ disease, chronic intestinal pseudoobstruction, scleroderma, and infiltrative diseases.
Chagas’ disease is endemic to Central and South America and is caused by a protozoan, Trypanosoma cruzi, which infects humans by a bite of an infected insect. The chronic form of the disease affects 10% to 20% of the patients who are infected and affects the colon, heart, and esophagus. The colon is most commonly affected, presenting as megacolon and, in some cases, sigmoid volvulus. The cardiac manifestations include cardiac arrhythmia and cardiomegaly. The esophageal manifestation includes megaesophagus. In addition, the disease may also cause destruction of the myenteric plexus of the duodenum and ureter. The diagnosis of Chagas’ disease is confirmed by detection of antibodies by complement fixation or immunofluorescence.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


