Aberrant Right Subclavian Artery
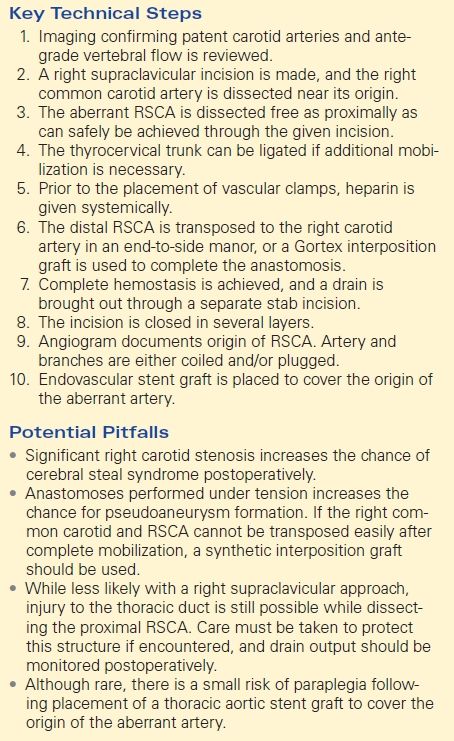
NICOLAS H. POPE and GILBERT R. UPCHURCH Jr
Presentation
A 35-year-old female presented to her primary care physician complaining of dysphagia to solid food. Her past medical history and physical examination were unremarkable. Noninvasive blood pressure measurements were equal in both upper extremities. A barium swallow study was ordered and demonstrated a posterior filling defect consistent with external compression of the esophagus (Fig. 1). Upper endoscopy revealed no mucosal pathology and a posterior, pulsatile, extraluminal mass in the proximal esophagus with significant narrowing of the esophageal lumen. Mannometric studies done at this time were unremarkable, and no biopsies were taken.

FIGURE 1 Upper gastrointestinal barium swallow demonstrating contrast filling defect in the proximal esophagus (arrow).
Differential Diagnosis
The differential diagnosis of dysphagia is broad and includes both benign and malignant esophageal tumors, mechanical esophageal pathologies such as Zenker ’s diverticulum, benign esophageal strictures, webs or rings, peristaltic and neuromuscular disorders, and extrinsic compression of the esophagus by other mediastinal masses or vascular structures. Given the findings of pulsatile external compression, a retroesophageal aberrant right subclavian artery (RSCA) should be highly suspected as a cause for this patient’s symptoms.
Discussion
Aberrant right subclavian (RSCA), or Lusorian artery, is a common variant of normal aortic arch anatomy, occurring in 0.5% to 1.0% of the population. It is thought to be the result of obliteration of the right fourth aortic arch during development. The RSCA then originates at an aortic diverticulum first described by Kommeral distal to the left subclavian. From there, it takes a variable course across the mediastinum to the right upper extremity. Retroesophageal Lusorian artery may present with dysphagia, as in the case presented. Workup of dysphagia begins with a barium swallow and EGD to look for more common pathologies. When a Lusorian artery is suspected, angiography has historically been the goldstandard for diagnosis. This has largely been replaced by computed tomography angiography, as it is noninvasive and allows for visualization of the entire mediastinum. Lusorian artery aneurysms are present in up to 60% of aberrant RSCAs and should uniformly be repaired, as the incidence of rupture is high.
Case Continued
CT angiography was performed (Fig. 2).
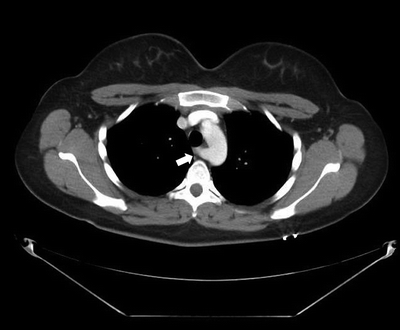
FIGURE 2 CTA demonstrating retroesophageal course of an aberrant right subclavian (Lusorian) artery (arrow).
Diagnosis and Recommendation
The diagnosis is aberrant origin RSCA with clinically significant compression of the esophagus. Traditionally, this requires open transposition through a right supraclavicular and sternotomy incisions and reanastomosis to the left carotid artery in an end-to-side manner. Advances in endovascular therapy have allowed for a less-invasive treatment option through a hybrid approach. This involves right carotid-subclavian bypass to revascularize the right upper extremity followed by occlusion of the origin of the aberrant artery with Amplatz occlusion device and covering of the ostium with a covered stent graft. Relief from dysphagia symptoms is typically excellent once flow in the retroesophageal portion of the artery is eliminated by either open or endovascular approach (Table 1).
TABLE 1. Aberrant Right Subclavian Artery
Treatment Approach
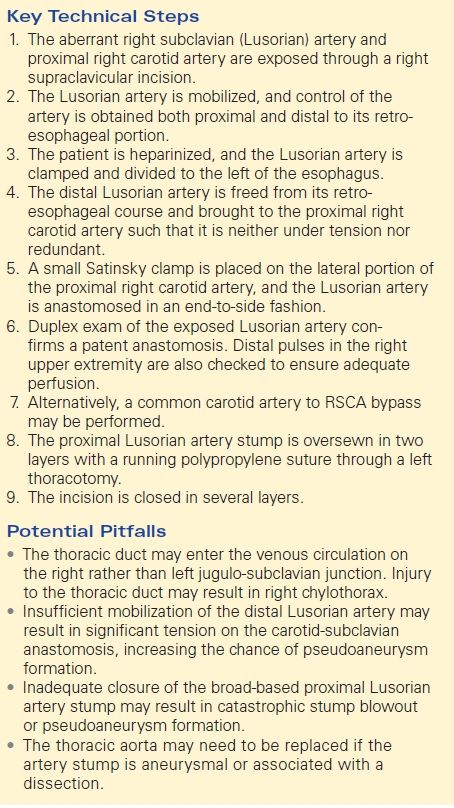
Open Surgical Repair
Open repair of a nonaneurysmal Lusorian artery involves transposition of the distal portion of the aberrant subclavian artery with reanastomosis to the right carotid artery to supply the right upper extremity. A prosthetic graft may be used to complete the carotid-subclavian bypass if there is difficulty mobilizing sufficient length of Lusorian artery to complete a tension-free anastomosis. Next, ligation of the proximal Lusorian artery proximal to its retroesophageal course is performed. This is accomplished through a left thoracotomy. The Lusorian artery is identified and mobilized both proximal to its retroesophageal course. The proximal portion of the artery to the left of the esophagus is oversewn in two layers with polypropylene suture. Care must be taken not to injure the thoracic duct, which may enter the right jugulo-subclavian commissure in these patients.
Hybrid Approach
Subclavian Revascularization
After discussion with the patient, she elects to proceed with carotid-subclavian bypass and endovascular occlusion. Preoperatively, a CTA of the head and neck is performed to ensure adequate flow to support the additional burden of the proposed bypass and avoid steal phenomena. She is brought to the hybrid suite and positioned in the supine position. General endotracheal anesthesia is induced, and a right carotid-subclavian bypass is performed through a supraclavicular incision. Bypass can be accomplished either by direct transposition or with a synthetic interposition graft. The thyrocervical trunk may be ligated if necessary to allow better mobilization of the proximal RSCA prior to beginning the anastomoses. The patient is heparinized prior to placement of vascular clamps. Transposition is completed in an end-to-side fashion with running polypropylene suture. Once complete, on-table Doppler exam can confirm adequacy and direction of flow. The field is inspected for hemostasis, and a drain is left in the wound bed (Table 2).
TABLE 2. Hybrid Technique