CARDIAC IMAGE INTEGRATION
Case presented by:
Question No. 1: Which of the following is true about integration of cardiac images?
A.Cardiac image integration (registration) is a rigid body registration as shown in Figure 76.1.
B.Cardiac motion and respiration can affect cardiac image integration.
C.Only 3D–3D image integration is possible.
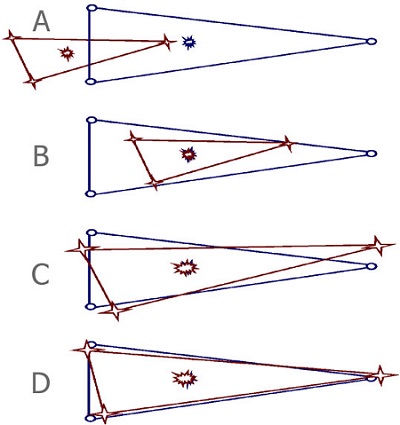
Figure 76.1. Simplified rigid body registration process. Panel A represents projection of computed tomography (CT) and reference image. Panel B depicts initial step, which involves translation of centroids. Panel C involves scaling to calibrate both images. Panel D shows rotation of the image to minimize the sum of the squared distances between fiducial points.
Discussion
Due to lack of contrast differentiation between the area of interest and surrounding structures in a moving structure like the heart, and as there is a lack of proper intraprocedure guidance using current imaging techniques for ablation, cardiac image registration using CT, magnetic resonance imaging (MRI), ultrasound, and fluoroscopy is currently being investigated and clinically used for atrial fibrillation (AF) ablation. Cardiac image registration, in the context of left atrium (LA), is intermodal, with the acquired image and the real-time reference image residing in different image spaces, and involves optimization in which one image space is transformed into the other. Geometry-based methods, which include using fiducial points and/or surface-based techniques, are usually used for cardiac image registration. During fiducial point registration, fiducial points are either external skin markers or manually determined by marking anatomical landmarks, using mapping catheters. Usually, a minimum of 3 noncollinear points are needed for optimal registration. Recently, a catheter placed inside the coronary sinus (CS) has also been used as a fiducial marker for the purpose of registration. During surface registration, the process involves characterizing surfaces in each of the images and deriving the best transformation between them. Unlike rigid body registration, such as has been extensively used in imaging the brain, cardiac image registration is unique and challenging. In addition to the errors inherent with intermodal registration, such as errors in pixel and voxel dimension and errors due to fiducial point selection, there are errors specific to cardiac image registration, that is, errors due to cardiac motion during the cardiac cycle and due to respiration.
Technical Considerations
Technical considerations regarding CT and MRI have been described in detail in previous cases. Cardiac registration, in the context of the LA, is intermodal, with the acquired images and real-time reference image residing in different imaged spaces. Registration algorithms involve the optimization of a cost function by the choice of a transformation T, which transforms one image space into the other. T can be either linear or nonlinear. Linear transformations are shape-preserving, and nonlinear transformations may deform both shape and size between images. A linear or nonlinear transformation decides the number of parameters involved in its definition. A linear transformation between three-dimensional (3D) spaces is defined by 6 parameters (or degrees of freedom), where 2 positions of a rigid body can always be related to one another in terms of 3 translations and 3 rotations. As the voxel sizes in each image may not be similar for calibration purposes, 3 extra degrees of freedom, equating to scaling in each direction, are needed. A nonlinear transformation, as it may deform both shape and size, will require more degrees of freedom.
Registration methods fall into 2 broad categories, those based on either geometric similarities between images or voxel-intensity similarities. Voxel-similarity methods are usually used to assess progression of disease. Geometry-based methods can be point-based or surface methods applied to both 3D–3D or 3D–2D registration methods.
Point-based registration methods depend on the appropriate definition of 2 sets of corresponding fiducial points in each set of images to be registered. Thus, if {xi}1N denotes the set of fiducial points in the acquired image, {yi}1N denotes the corresponding points on the real-time image, that is, the choice of T minimizes the error ∑iN=1 IIτ(x)-y1 II2. Fiducial point sets are either automatically determined based on external skin markers or manually determined based on anatomical landmarks. The latter method has been used in cardiac image registration. For rigid structures such as the brain, 3 noncollinear fiducial points may be sufficient to establish the transformation between the 3D image volumes. However, the larger the number of points used, the more any error occurring during collection of the points is averaged out. The algorithm for calculating the transformation between the 3D images involves first computing the average of the “centroids” of each set of points. The difference between the centroids in the 3D images tells us the translation that must be applied to one set of points. These points are then rotated about the new centroid until the sum of the squared distances between each corresponding point pair is minimized. The square root of the mean of this squared distance is referred to as fiducial registration error (FRE).
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


