CARDIAC RESYNCHRONIZATION THERAPY IN CONGENITAL HEART DISEASE
Case presented by:
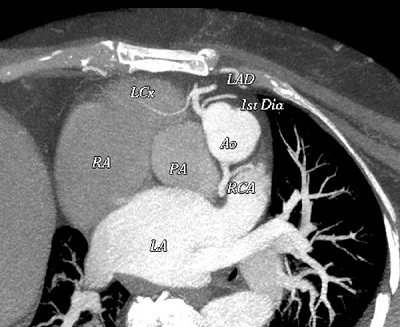
A 51-year-old woman with asymptomatic congenital heart disease (left ventricular ejection fraction [LVEF] 64%) underwent chemotherapy with doxorubicin (Adriamycin) for breast cancer. Four weeks after completing chemotherapy, she presented with atrial fibrillation (AF), a rapid ventricular response, and heart failure. She was treated with amiodarone, digoxin, beta-blockers, and warfarin. One week later, she developed complete heart block with a junctional escape rhythm at 45 bpm, and worsening heart failure. Systemic LVEF was now 25%. Cardiac computed tomography (CT) was obtained (Figure 66.1).
Question No. 1: The best course of action is:
A.Insert temporary pacemaker and stop amiodarone; await recovery of atrioventricular (AV) conduction.
B.Implant dual-chamber implantable cardioverter-defibrillator (ICD).
C.Implant transvenous cardiac resynchronization therapy-defibrillator (CRT-D).
D.Implant CRT-D with epicardial lead via thoracotomy.
Panel A
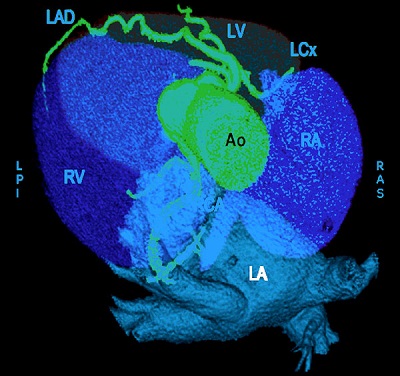
Figure 66.1. Cardiac CT images showing location and course of the coronary sinus (CS), and coronary arteries (CA). A: The right (RV) and left ventricles (LV) were transposed as were the aorta (Ao) and pulmonary arteries (PA). The systemic LV was dilated (LVEF 30%). B: The CS was small and followed the course of the right coronary artery (RCA). LA, left atrium; LAD, left anterior descending artery; LCx, left circumflex artery; RA, right atrium.
Discussion
Congenitally corrected transposition of the great vessels (CCTGV) accounts for less than 1% of congenital heart disease. It is usually associated with a ventricular septal defect or pulmonic stenosis, and survival depends upon the severity of the associated abnormalities. CCTGV without associated abnormalities is a very rare condition1 and patients can survive up to middle or even old age.2 Death usually occurs due to heart failure or complete heart block; the latter condition occurs in 10% of patients even without Adriamycin-induced cardiomyopathy.3 Thus, implantation of a temporary pacemaker and discontinuing amiodarone is unlikely to resolve the heart block, and recurrence of AF is likely in the absence of antiarrhythmic therapy.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


