LEFT VENTRICULAR LEAD PLACEMENT IN CARDIAC RESYNCHRONIZATION THERAPY
Case presented by:
A 63-year-old male presents for consideration of cardiac resynchronization therapy (CRT) upgrade. He has a history of ischemic heart disease and clinical heart failure with several admissions for acute decompensation in the past 2 years. At present, he is at his baseline volume status with ambulatory NYHA class IV symptoms. He denies any current chest pain or other signs of active ischemia, and his other chronic medical conditions (diabetes mellitus, hyperlipidemia, and sleep apnea) are controlled on good therapies. For his heart failure the patient is on carvedilol, lisinopril, spironolactone, and furosemide.
Reviewing objective data shows a recent echocardiogram with severe global hypokinesis of the left ventricle (LV) and an ejection fraction of 15% to 20%. His surface ECG is shown in Figure 60.1. His past surgical history is notable for two-vessel coronary bypass grafting 7 years ago.
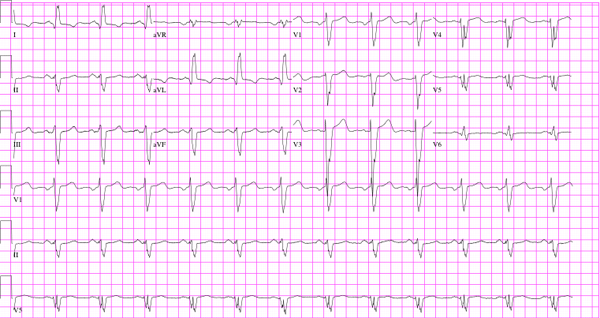
Figure 60.1. Patient’s surface ECG at presentation.
A.Main coronary sinus (CS).
B.Middle cardiac vein.
C.Any position within the coronary venous system with low threshold values.
D.Anterior cardiac vein.
A.QRS duration < 150 ms.
B.Evidence of lateral infarct.
C.Prior bypass surgery.
D.Severity of LV hypokinesis on echocardiography.
Question No. 3: Which of the following tests may assist in the pre-implant process?
A.Computed tomographic (CT) angiogram.
B.Viability assessment.
C.CT venogram.
D.Cardiac magnetic resonance imaging (MRI).
A.True.
B.False.
Discussion
Successful delivery of CRT is dependent on many factors. After selecting an appropriate patient (as outlined in the previous case), technical issues during implantation need to be considered. Typically, right atrial and right ventricular (RV) leads are placed in a fashion similar to standard dual-chamber device implants, via the venous system (generally accessed via the subclavian or axillary veins). The same access site is then used for the introduction of the LV lead. However, appropriately placing the LV lead can be challenging.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


