MULTIMODALITY APPROACH TO DIAGNOSING ARRHYTHMOGENIC RIGHT VENTRICULAR DYSPLASIA
Case presented by:
A 25-year-old male runs on the cross-country team for his college. He has had a long history of palpitation and rapid heart beating. He experienced a recent episode of complete syncope preceded by a rapid heart beat.
Question No. 1: The ECG in Figure 47.1 reveals:
A.Inferior ischemia.
B.Intraventricular conduction delay.
C.Evidence of a genetic cardiomyopathy.
D.Wolff-Parkinson-White syndrome.
E.Long QT syndrome.
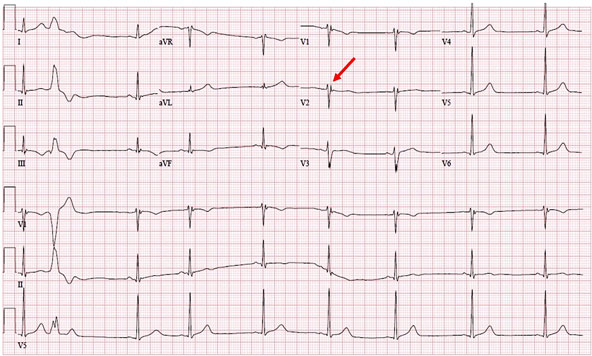
Figure 47.1a. Patient’s ECG at baseline. See zoomed image for further detail.
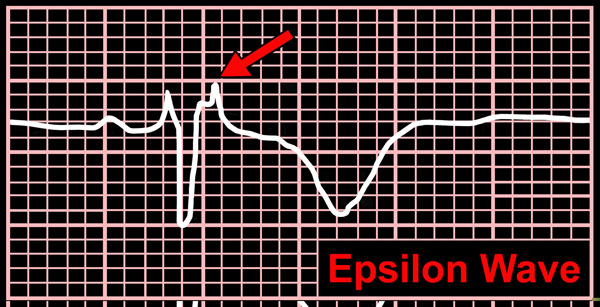
Figure 47.1b. (zoomed in). Patient’s ECG displaying an epsilon wave (red arrow).
Discussion/Follow-up Questions
Epsilon waves are caused by postexcitation of myocytes in the right ventricle (RV). Young patients with ventricular tachycardia (VT) or syncope and epsilon waves on electrocardiography (ECG) usually have arrhythmogenic right ventricular dysplasia (ARVD). In this condition myocytes are replaced by fat, producing islands of myocytes surrounded by variable fat. This causes the delay in excitation of some of the myocytes of the RV and causes the little “wiggles” seen during the ST segment of the ECG.
Epsilon waves have also been described in patients with posterior infarction, sickle cell disease with RV hypertrophy due to pulmonary hypertension, RV infarction, sarcoidosis, and infiltrative disease of the RV.
Question No. 2: Which of the following is/are true?
A.The epsilon wave on the ECG is diagnostic of ARVD.
B.The epsilon wave occurs in 100% of cases of ARVD.
C.There are T-wave inversions in the V1 to V3 leads in 75% of cases of ARVD.
D.The ECG is frequently normal despite evidence of ARVD.
E.A and D are correct.
F.None are correct.
Diagnosis of ARVD involves the presence of various combinations of electrocardiographic (Table 47.1), structural and functional abnormalities, and a family history of the disease. Epsilon waves in leads V1 to V3 are a hallmark of the disease and occur in 30% of patients; 50% of patients have T-wave inversion in right precordial leads. (See also case no. 50)
Table 47.1. Diagnostic Criteria that can be Diagnosed on Electrocardiography (ECG)
1.(major) Epsilon wave or localized prolongation (>110 ms) of the QRS complex in right precordial leads (V1 to V3) 2.(minor) Inverted T waves in right precordial leads (V2 and V3) (people aged more than 12 years); in absence of right bundle branch block (RBBB) 3.(minor) Late potentials (signal-averaged ECG) 4.(minor) Left bundle branch block (LBBB)-type VT (sustained and nonsustained) (ECG, Holter, and exercise testing) 5.(minor) Frequent ventricular extrasystoles (more than 1000/24 hours) (Holter) |
Question No. 3: Which of the following is/are true?
A.Incidence of the disease is approximately 1:3000 to 1:10,000.
B.ARVD is a progressive disease.
C.ARVD is felt to be mostly an autosomal dominant disease.
D.Naxos disease is a unique from of ARVD and is autosomal recessive.
E.ARVD frequently manifests in young males.
F.All are true.
G.Three are true.
ARVD is characterized by fatty replacement and fibrosis of the heart. Most commonly, the right ventricle apex (RVA) and outflow tract are involved. However, the left ventricle (LV) can be affected to. As a result of the fatty replacement and fibrosis, ventricular arrhythmias are common in this disease and can lead to palpitations, syncope, and sudden death. At more advanced ages, right ventricular pump failure can occur.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


