NEWER ORAL ANTICOAGULANTS IN ATRIAL FIBRILLATION
Case presented by:
A 76-year-old woman is referred to discuss anticoagulation therapy for paroxysmal atrial fibrillation (AF). She had initially presented with AF 3 years earlier and indicates her episodes occur 4 to 5 times monthly and last 15 to 30 minutes. Her medical history also includes hypertension, dyslipidemia, former tobacco abuse, and peripheral vascular disease with a history of claudication symptoms in her left lower extremity. Her current medications include a daily aspirin (81 mg), losartan 100 mg daily, metoprolol 50 mg twice daily, and simvastatin 20 mg nightly. She has a structurally normal heart by transthoracic echocardiography. At the time of her office visit, she is in sinus rhythm with a heart rate of 65 bpm and her blood pressure is 130/85 mmHg. Her cardiac examination is normal with no murmurs or gallop and there are no signs of congestive heart failure. A bruit is heard over the left femoral artery.
You determine that the patient has a CHADS2 risk score of 2 and, therefore, warrants systemic anticoagulation. The patient expresses reluctance to start warfarin since she wants to avoid the need for frequent blood tests.
Question No. 1: Does patient need anticoagulation therapy?
A.True.
B.False.
Question No. 2: What current and future alternatives to warfarin may be available for this patient?
Discussion
AF confers an approximate fivefold increased risk of stroke, which is a major cause of disability and a leading cause of death among patients with AF. The vast majority of these strokes are cardioembolic. Systemic anticoagulation with warfarin has been the cornerstone of therapy for stroke prevention among patients who have a definite indication for anticoagulation (eg, patients with a CHADS2 risk score of ≥ 2) and no contraindication. Treatment with warfarin provides a 60% to 70% reduction in stroke risk compared with no therapy and confers a 30% to 40% risk reduction when compared with aspirin. Despite its efficacy, warfarin has important limitations. The anticoagulant effects of the drug must be monitored regularly to ensure adequate stroke prevention, interactions with food and other drugs hamper its use, and the drug has a narrow therapeutic range. In randomized, controlled trials, patients treated with warfarin have a therapeutic international normalized ratio (INR) only two-third of the time. In routine clinical practice, an even lower percentage of patients are in range, leaving patients relatively unprotected from thromboembolic complications.2 An alternative to warfarin would clearly be desired.
New oral anticoagulants now undergoing trials for AF generally have different targets in the anticoagulation cascade than the vitamin K-dependent clotting factors inhibited by warfarin (Figure 51.1). The new oral anticoagulants closest to general release segregate into 2 classes: a direct thrombin (factor IIa) inhibitor (dabigatran) and direct factor Xa inhibitors (rivaroxaban, apixaban, betrixaban, and edoxaban).
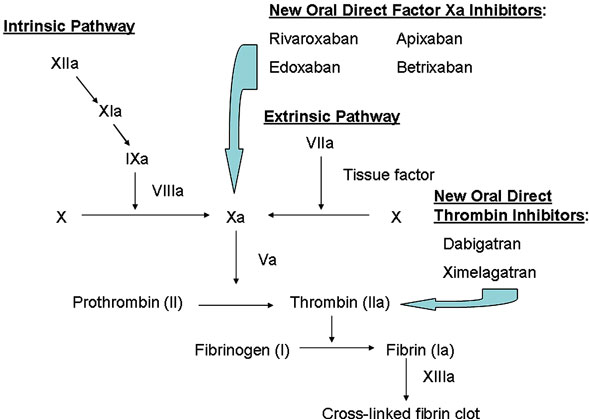
Figure 51.1. Site of action of newer anticoagulants.
Direct Thrombin Inhibitors
Direct thrombin inhibitors have a variety of effects on the coagulation cascade.3 By inhibiting thrombin activation, the conversion of fibrinogen to fibrin is attenuated. Additional effects include the inhibition of thrombin-mediated activation of clotting factors V, VIII, XI, and XIII as well as the prevention of thrombin-mediated platelet activation. Ximelagatran was the first oral direct thrombin inhibitor studied for stroke prevention in patients with nonvalvular AF. Ximelagatran was shown to be noninferior to warfarin in both efficacy and safety end points.4,5 However, a potentially higher risk for drug-induced liver injury with ximelagatran prompted its withdrawal from all markets and halted further development of the drug.
A second oral direct thrombin inhibitor, dabigatran, has recently completed clinical trials and has been approved for use in the United States by the Food and Drug Administration (FDA). Dabigatran is a reversible direct inhibitor of thrombin with a rapid onset of action and 6.5% oral bioavailability not affected by food intake.3
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


