FRAGMENTED QRS
Case presented by:
A 55-year-old man with history of diabetes, hypertension, and hyperlipidemia presented with atypical chest discomfort. He denied any history of chest pain and did not receive any specific therapy for coronary artery disease (CAD) in the past. Examination revealed an obese gentleman with blood pressure of 142/88 mmHg and a heart rate of 75 beats per minute. Physical examination including lung and cardiac exam was unremarkable. He is on aspirin and lisinopril. An ECG was obtained in the emergency department and is shown in Figure 43.1.
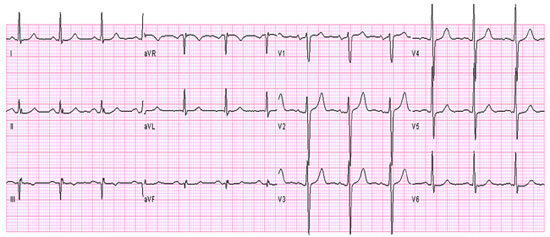
Figure 43.1 ECG on presentation.
Question No. 1: The ECG in Figure 43.1 shows:
A.Acute myocardial infarction (AMI).
B.Interventricular conduction delay.
C.Fragmented QRS (fQRS).
D.Nonspecific ST-T wave abnormality.
Question No. 2: Which of the following is associated with the abnormality in the above ECG (see Figure 43.1)?
A.Myocardial scar.
B.Arrhythmogenic right ventricular dysplasia (ARVD).
C.Brugada Syndrome.
D.All of the above.
Question No. 3: The abnormality in the above ECG (see Figure 43.1) predicts which of the following in patients with ischemic cardiomyopathy?
A.All-cause mortality.
B.Cardiac mortality.
C.Arrhythmic events (ICD therapy).
D.All of the above.
The patient’s chest pain was relieved by oral nitroglycerine. Three sets of cardiac markers were within normal limits. The patient underwent myocardial perfusion single photon emission computed tomography (SPECT) that revealed a fixed perfusion defect in the right coronary artery (RCA) territory (Figure 43.2).
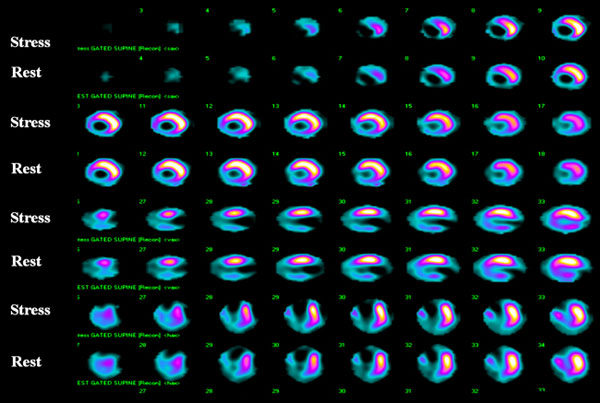
Figure 43.2 Myocardial perfusion SPECT depicting a fixed perfusion defect in the RCA territory.
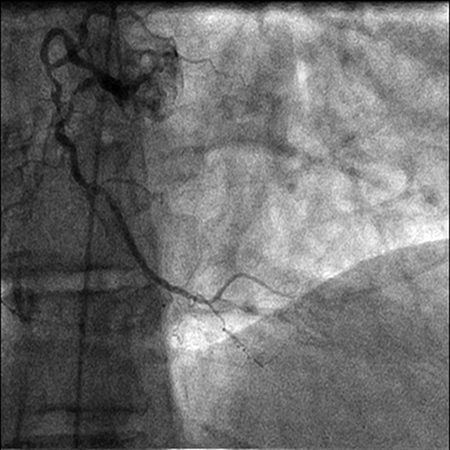
A coronary angiogram was later performed that showed single-vessel CAD with an occluded RCA (Figures 43.3 and 43.4).
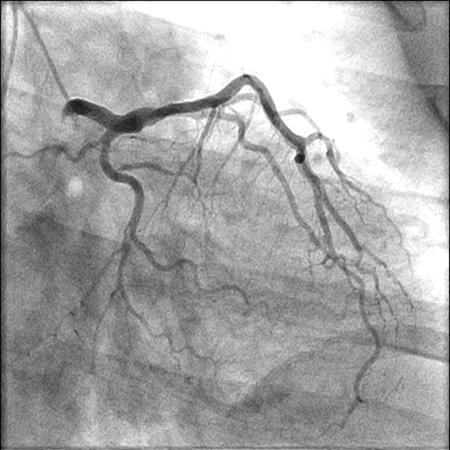
Figure 43.3 Coronary angiogram of the left coronary system showing patent coronary arteries.
fQRS is defined as unexpected deviations in the QRS morphology on a 12-lead ECG. fQRS includes various RSR′ morphologies (see Figure 43.5) of the QRS complex with or without a Q wave and is defined by the presence of an additional R wave (R′ or R prime), or notching in the terminal portion of the S wave, notching of R wave or the presence of more than one R′ in 2 contiguous leads corresponding to a major coronary artery territory.1 It is postulated that regional myocardial scar, which is associated with alterations in QRS morphology, causes terminal conduction delay, which is appreciated as fragmentation of QRS complexes.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


