BRUGADA SYNDROME: DIFFERENT PRESENTATIONS
Case presented by:
First Case
A 68-year-old man who presented with palpitations and dizziness was noted to be in atrial fibrillation (AF) with fast ventricular rate, which spontaneously converted to sinus rhythm. An ECG obtained after conversion to sinus rhythm is shown in Figure 42.1. His past medical history included hypertension, which was well-controlled on cardiazem (240 mg daily). He was a nondiabetic smoker with no prior history of coronary artery disease, myocardial infarction (MI), congestive heart failure (CHF), syncope, transient ischemic attack, or cerebrovascular accident. His echocardiogram revealed normal left ventricular ejection fraction (LVEF) with no valve disease, and his cardiac catheterization revealed normal coronaries. The patient was on no other medications and his blood chemistries, cell count, and thyroid-stimulating hormone test were all normal. He was initiated on flecainide (100 mg orally twice daily) for suppression of paroxysmal AF and discharged home.
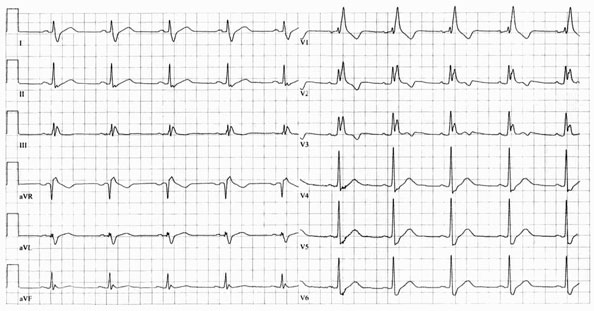
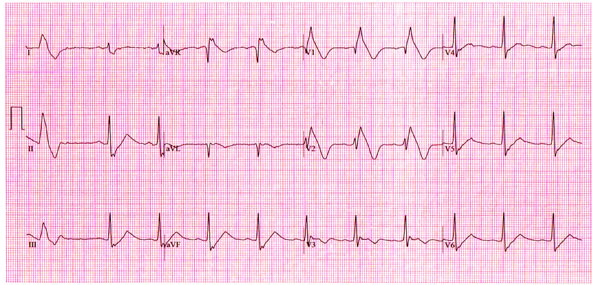
Figure 42.2 Follow-up ECG at 2-week posthospitalization visit.
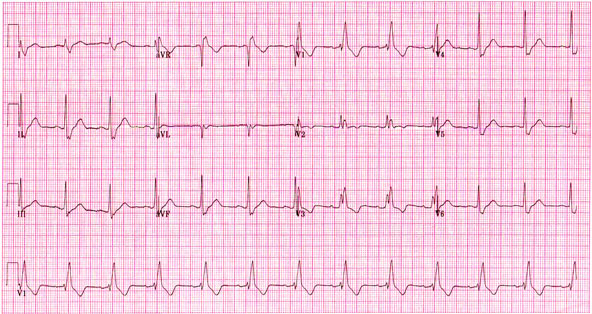
Figure 42.3 ECG obtained 2 weeks following the previous follow-up ECG (Figure 42.2).
Question No. 1: What is the most likely cause of the abnormality seen in the ECG shown in Figure 42.2?
A.Combined INa and ICa blockade leading to unmasking of underlying Brugada syndrome.
B.Flecainide toxicity.
C.Increased levels of calcium channel blocker due to drug interaction.
D.Acute pulmonary embolism from right atrial thrombus dislodgement.
Discussion
The typical ECG appearance (see Figure 42.2) is that of Brugada syndrome. Mutations in SCN5A associated with a loss of function of the sodium channel have been shown in up to 20% of patients with Brugada syndrome. This is consistent with the clinical finding that potent sodium channel blockers of class IC antiarrhythmic agents, such as flecainide, ajmaline or pilsicainide or class IA agents such as procainamide and disopyramide, can unmask the Brugada syndrome when the baseline ECG is normal. It has been shown, in vitro, that a combination of sodium and calcium channel block is much more effective in precipitating the ECG manifestation of Brugada syndrome experimentally.
Clinically, a variety of drugs have been used to unmask the so-called Type1 Brugada ECG pattern. Two of the commonly used drugs studied, flecainide and ajmaline, have shown variable sensitivity and specificity. Ajmaline (not available in United States) showed a sensitivity of 80%, specificity of 94%, and a negative predictive value of 83%. Flecainide showed a much lower negative predictive value of 36%, with sensitivity and specificity of about 80%. In light of these findings, ajmaline is more effective in unmasking Brugada syndrome.
A positive response to a sodium channel blocker is characterized by the following (Figure 42.3):
- Type 1-coving ST-segment elevation in leadsV1, V2, or V3
- Conversion of Type 2 or Type 3 to Type 1 pattern.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


