CATHETER ABLATION FOR LONG-STANDING PERSISTENT AF
Case presented by:
A 64-year-old hypertensive gentleman presented with symptomatic, 5-year-long permanent, drug-refractory atrial fibrillation (AF). Patient complained of dyspnea and effort intolerance—NYHA class II despite good rate control therapy. He was diagnosed with paroxysmal AF at age 30. Echocardiographic left atrial (LA) size was 49 mm and left ventricular ejection fraction was 58%. 12-lead ECG is shown in Figure 27.1.
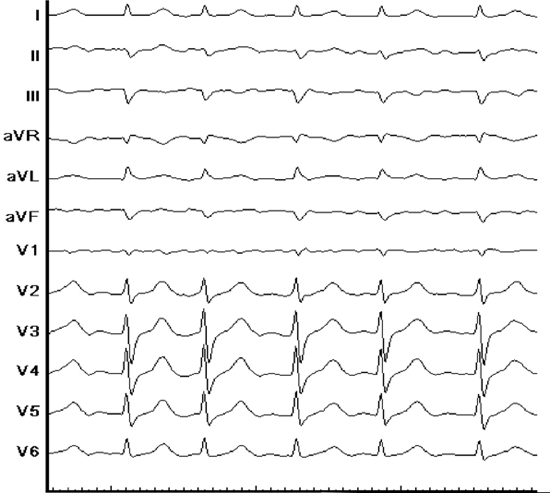
Figure 27.1 Baseline 12-lead ECG.
Question No. 1: What are the procedural end points of stepwise ablation approach?
Question No. 2: What are the critical structures for termination of AF during stepwise ablation?
Question No. 3: What are the short and long term clinical outcomes of stepwise ablation?
Question No. 4: What are the characteristics of arrhythmia recurring after stepwise ablation?
Discussion
Certain baseline electrocardiographic parameters can predict the procedural complexity and response to ablation in persistent AF. These parameters include: baseline average global fibrillatory cycle length (CL) in leads with best visible fibrillatory (F) waves’ usually magnified lead V1; and baseline average amplitude of the F wave measured in magnified leads II and V1.1 Ten discrete F waves were selected during a period of slow ventricular rate to avoid superimposition of QRST, and measurements were performed using electronic calipers.
After intracardiac introduction of the catheters, baseline atrial fibrillatory cycle length (AFCL) was measured simultaneously with the Lasso catheter in the left atrial appendage (LAA) and the mapping (ablation) catheter in the right atrial appendage (RAA), averaging a recording of at least 10 consecutive cycles to obtain local AFCL in the 2 chambers. Baseline LAA AFCL was 146 ms and RAA AFCL was 143 ms.
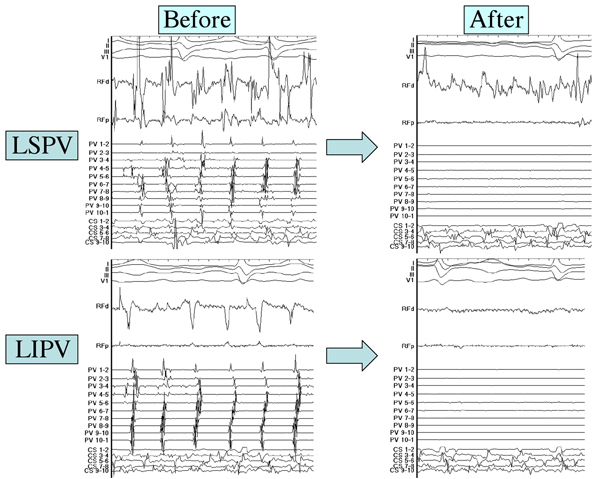
Figure 27.2. Example of left pulmonary vein isolation (PVI).
Using stepwise approach for persistent AF ablation, 4 pulmonary veins were isolated at first. Circumferential PVI was performed in a 2 × 2 manner, encircling 2 ipsilateral veins together under the guidance of a single Lasso catheter. Figure 27.2 shows left PVI. The procedural time for PVI was 50 minutes, with radiofrequency duration of 42 minutes and fluoroscopic time of 16 minutes.
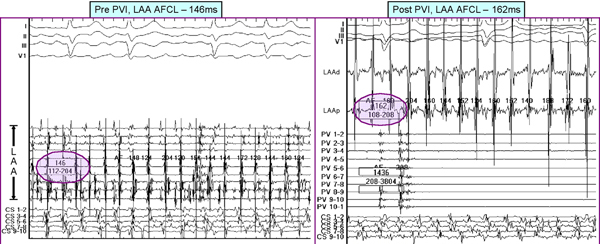
Figure 27.3. LAA AFCL both pre- and post-PVI.
Following PVI, AFCL was measured in the LAA/RAA regionally. LAA AFCL rose by 16 ms after successful PVI as shown in Figure 27.3. High gradient between local AFCLs recorded from the pulmonary vein and the LAA before ablation can substantially impact the regional and global AFCL after PVI.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


