EMBRYOLOGY AND ANATOMY
OF THE ATRIAL SEPTUM
SIEW YEN HO
Increasingly, transcatheter interventional procedures require access to the left heart chambers via the atrial septum. To ensure that these procedures are successful and to reduce the risk of complications, a detailed knowledge and understanding of the atrial septum, which separates the left and right atrial chambers, is crucial. While morphologists can view the heart from all angles and display the atrial septum to best advantage, their views sometimes differ from those commonly used by interventional electrophysiologists. Adopting McAlpine’s attitudinal approach for describing the locations of the heart’s structures can improve our understanding of its anatomy.1 Nevertheless, there remains the issue of speaking a common language. The terminology used when describing cardiac embryogenesis is confusing because, historically, the same structures have been given different names, and eponyms are rather common.2 Furthermore, the conversion of Latin terms into English, while laudable for readers who are fluent in English, can be confusing for others.
Echoing Whitmore’s sentiments in “Terminologia Anatomica: New Terminology for the New Anatomist” that terminology must accommodate all users, I hope the terminology used in this chapter will suit cardiologists, morphologists, and scientists alike.3 Latinate terms will be offered in association with their commonly used English equivalents. The first part of this chapter is a review of the embryologie development of the atrial septum. As this section is meant to enhance the understanding of structures in the definitive heart, I will use attitudinal orientations as much as possible when describing those locations. The bending and growth of the heart tube during development continually shifts these structures, however, so their locations can be described only in general terms. Traditionally, embryologists use ventral, dorsal, cephalad, and caudad as their compass points because those terms can be applied to both bipeds and quadrupeds. I prefer the terms anterior, posterior, superior, and inferior, respectively, which are more compatible with descriptions of the human postnatal heart.
Developmental Anatomy
At the early stages of cardiac development, the embryonic hearxt tube is more or less straight with a venous pole at the inferior end and an arterial pole at the superior end. The tube is attached posteriorly along its length by mesocardium to the body of the embryo. This tube gives rise to the ventricles and, through the process of looping, detaches much of its length from the mesocardium. During the looping process, the inferior pole, which is also the inlet part of the tube, expands to form the atrial component, concomitant with the expansion of the superior pole, the outlet portion, through recruitment of extracardiac cells. Wide venous channels, which carry blood from both the right and left sides of the embryo back to the heart, connect to the developing atrial portion. The paired veins form the so-called horns of the sinus venosus. The common cardinal veins (ducts of Cuvier) drain from each side of the embryo into the sinus, as do the umbilical veins from the placenta and the vitelline veins from the yolk sac.
At the fourth week of development, there are no anatomical borders between the sinus venosus and the primitive atrium. The sinus venosus portion becomes asymmetrical as the left horn diminishes in size and is incorporated into the developing left atrioventricular junction, while the right horn grows rapidly. The left horn, which ultimately receives only the left duct of Cuvier, persists as the coronary sinus. Consequently, the entire systemic venous component opens to the right portion of the primitive atrium, which, in turn, continues to the developing atrioventricular junction at the atrioventricular canal (Figure 2.1a).
While the primitive atrium is developing, endocardial cushions form within the canal in preparation for the remodelling of the atrioventricular junction and cardiac sep-tation (Figure 2.1b). Two cushions, the superior and inferior cushions, project into the lumen; they meet in the middle, dividing the common orifice of the canal into right and left orifices. The union of the endocardial cushions is thought to form the septum intermedium, but the cushions are not the only contributors to septation of the atrioventricular canal (discussed below).
The remaining systemic veins remodel. The vitelline and umbilical veins become a single vessel, the inferior caval vein (inferior vena cava). Thus, the venous component, which includes the entrances of three veins, the inferior caval vein and the right and left ducts of Cuvier, opens into the posterior aspect of the primitive atrium. Valve-like structures develop to the right and left sides of the venous component to demarcate its junction with the atrium, allowing anatomical distinction between the sinus venosus and the primitive atrium. These valves, described as the right and left venous valves, fuse at their superior and inferior extremities (Figure 2.1a). The right venous valve continues into the pos-terosuperior wall of the atrium, forming the septum spurium, which, as the name suggests, is a false septum because it reaches its fullest development during the third month and then diminishes to become the sagittal bundle in the formed heart. The posteroinferior wall of the sinus venosus folds inward to form the so-called sinus septum (eustachian ridge); this fold divides the right venous valve into two portions (Figure 2.1c). The valvar remnants become the eustachian and Thebesian valves, which guard the orifices of the inferior caval vein and the coronary sinus, respectively. The tendinous commissure between the two venous valves extends through the sinus septum, which later becomes the anteroinferior rim of the foramen ovale and a border for the triangle of Koch (discussed below). As the sinus venosus becomes incorporated into the primitive atrium, the left and right sides of the primitive atrium expand to form the atrial appendages. In the definitive heart, the right border between the sinus venosus and the atrial appendage is marked internally by the crista terminalis (terminal crest).
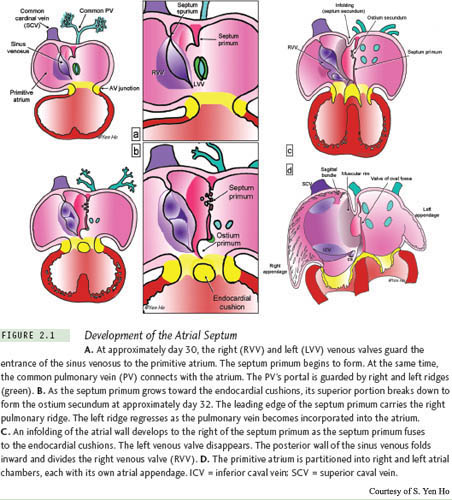
At the time when the primitive atrium begins to be partitioned, approximately day 30 of development, the lungs are just beginning to bud from the trachea, and a venous channel forms in the posterior mesocardium behind the heart. The venous channel becomes the common pulmonary vein that collects the pulmonary venous plexus into the posteroinferior part of the primitive atrium. The entrance of the common pulmonary vein is slightly to the left of the atrial midline, and it is bound on the right and left sides by ridges of persisting posterior mesocardium that protrude into the atrial cavity (Figure 2.1a). The right ridge, described as the spina vestibuli by His, develops to be more prominent and contributes to cardiac septation.4
The first sign of atrial septation is the appearance of the septum primum (primary septum) as a crescent of muscle in the atrial roof (Figures 2.1a, 2.1b). The inferior part of the septum primum is continuous with the spina vestibuli (vestibular spine, dorsal mesenchymal protrusion).5 This extends further and further into the cavity of the primitive atrium toward the endocardial cushions that are in the process of fusing to divide the atrioventricular canal into right and left portions. During this time, approximately day 32 of development, the atrioventricular canal expands rightward in readiness for connecting the developing right atrium to the distal part of the looped heart tube, which is to become the future right ventricle (Figure 2.1b). The leading margin of the septum primum is edged by mesenchyme (cells of mesodermal origin), which is thought to be derived from embryonic endocardium.6,7 The gap between the free edge of the septum primum and the fused superior and inferior atrioventricular endocardial cushions is the ostium primum (foramen primum or primary atrial foramen). With the incorporation of additional mesodermal tissue, the spina vestibuli expands, and, by approximately day 42 of development, combines with the septum primum and the endocardial cushions to ultimately close the ostium primum.8 This process carries the inferior ends of the venous valves anteriorly, and muscularization of the expanded spina vestibuli reinforces the base of the septum primum. The upper portion of the septum primum remains thin and persists as the flap valve of the definitive foramen ovale (Figure 2.1d). However, before the ostium primum can be fully obliterated, the upper portion of the septum primum, close to its origin at the atrial roof, breaks down to form the ostium secundum (foramen secundum, foramen ovale secundum, or secondary atrial foramen) (Figure 2.1c). The ostium secundum is important for the continuation of adequate blood flow to the left side of the heart after cardiac septation.
At approximately day 37 of development, the common pulmonary vein divides into left and right branches and becomes incorporated into the developing left atrium to form its posterior wall. The left pulmonary ridge disappears. Remodelling of the portion of roof of the atrium between the left venous valve that guards the entrance of the superior caval vein (superior vena cava) and the septum primum begins. To the right of the septum primum, the atrial wall folds inward to form the posterior, superior, and anterosuperior margins of the muscular rim (limbus fossa ovalis). This infolding is the septum secundum; it acts like a door frame, allowing the septum primum, or the “door,” to close against it after birth. The curved shape of the leading edge of the septum secundum demarcates the foramen ovale, which is analogous to the doorway. In the developed heart, this edge is described as the limbus (rim) of the foramen ovale. Unfortunately, as we shall see in a later section, there is some confusion regarding the term foramen ovale (oval foramen, fossa ovalis/oval fossa). The anterosuperior part of the infolding, together with the septum primum, separates the orifice of the superior caval vein from the orifice of the right superior pulmonary vein. The atrial walls expand inferiorly and posteriorly while the atrioventricular junction develops to incorporate the insulating fibrofatty tissue plane of the atrioventricular groove. This remodelling carries the newly muscularized spina vestibuli forward to form the anteroinferior margin of the muscular rim and the triangle of Koch.8 While the primitive atrium develops, the heart tube bends upon itself, ultimately bringing the outlet portion in front of the atria. The rapid growth of the atria and their appendages results in the anterior atrial walls appearing to embrace the outlet (Figure 2.1d). As the heart grows bigger, the ventricles become larger than the atria, and the aorta becomes the great artery that is closest to the anterior walls of the atria.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


