NODOFASCICULAR PATHWAY
Case presented by:
A 41-year-old gentleman presented with recurrent narrow-complex tachycardia, unresponsive to treatment with amiodarone or propafenone. The tachycardia was not terminable with adenosine, diltiazem, metoprolol, digoxin, and carotid sinus massage.
Question No. 1: The tracings shown in Figure 18.1 are most consistent with:
A.Atrioventricular nodal reentry tachycardia (AVNRT).
B.Atrial tachycardia (AT).
C.Junctional tachycardia.
D.Orthodromic atrioventricular reentry tachycardia (AVRT).
E.Orthodromic tachycardia involving a nodofascicular or a nodoventricular bypass tract.
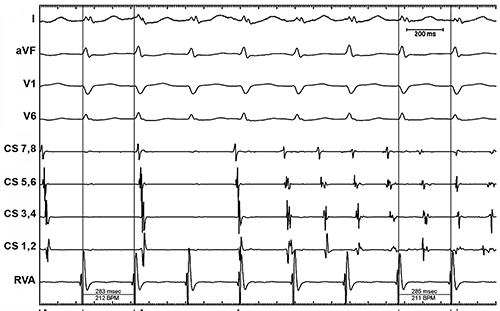
Figure 18.1. Tachycardia tracings.
Nodoventricular and Nodofascicular Bypass Tracts
In 1971, Wellens et al1 attributed the antegrade decremental conduction properties of atypical accessory pathways to their origin from the atrioventricular (AV) node. Atypical accessory pathways with decremental conduction were labeled as nodoventicular or nodofascicular pathways (Mahaim pathways). The tipping point was in 1988 when atriofascicular pathways were first described.2,3
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


