SLOW/FAST AVNRT: A GROUP OF 3 TACHYCARDIAS
Case presented by:
A 27-year-old woman was undergoing an attempt at catheter ablation of slow/fast atrioventricular nodal reentrant tachycardia (AVNRT). The diagnosis of slow/fast AVNRT was based on: the response to a single ventricular extrastimulus delivered to the para-Hisian region (retrograde atrial activation was not advanced until His-bundle [HB] activation was advanced); and the retrograde atrial activation sequence (earliest activation was recorded posterior to the tendon of Todaro [ToT]), at a superior-inferior level approximately halfway between the level of the site recording the most proximal HB potential and the level of the roof of the coronary sinus (CS) ostium1 (middle horizontal line in Figure 10.1A). Further, para-Hisian pacing (with intermittent His bundle-right bundle branch [HB-RB] capture), decremental ventricular pacing and ventricular extrastimulus testing demonstrated only retrograde fast atrioventricular (AV) nodal pathway conduction with the same atrial action sequence as the tachycardia (earliest activation was recorded posterior to the ToT). Not even a single beat of retrograde conduction over a slow AV nodal pathway was observed.
Linear radiofrequency (RF) ablation (continuous pullback, 40 W) was performed across the inferior triangle of Koch, between the tricuspid annulus (TA) and CS ostium at the level of the middle of the CS ostium (line #1, see Figure 10.1A), producing vigorous accelerated junctional rhythm (with retrograde fast pathway conduction) at 2 sites along the line. An ASP potential (activation recorded between the TA and CS ostium in the inferior-to-superior direction, Figure 10.3A) continued to be recorded inferior to the ablation line, but not superior to the ablation line. Sustained slow/fast AVNRT continued to be induced, with no change in tachycardia cycle length (TCL), AH interval, or HA interval. There was also no change during decremental atrial pacing in the shortest atrial pacing cycle length, maintaining 1:1 antegrade conduction over the fast pathway or slow pathway.
A second RF ablation line was created between the TA and CS ostium at the level of the roof of the CS ostium (line #2, see Figure 10.1A). Accelerated junctional rhythm occurred at one of the sites during the linear RF application. Sustained slow/fast AVNRT was again induced with the same TCL, AH interval, and HA interval. Ablation was not attempted within the triangle of Koch further superior than the level of the roof of the CS ostium.
Next attempted was a linear RF application along the roof of the CS as a pullback (RF power 15-20 W), beginning approximately 4 to 5 cm from the CS ostium and continuing until approximately 1 cm from the CS ostium (line #3, see Figure 10.1B. There was no accelerated junctional rhythm during that RF application. Sustained AVNRT remained inducible. The ablation line along the roof of the CS was extended to the CS ostium, and then along the superior half of the apical edge of the CS ostium (line #3, see Figure 10.1B). Sustained slow/fast AVNRT continued to be induced with the same TCL, AH interval, and HA interval. There was still no change in the shortest atrial pacing cycle length, maintaining 1:1 antegrade conduction over the fast pathway or slow pathway.
How could you now locate and ablate (with the least risk of AV block) the slow AV nodal pathway forming the antegrade limb of this reentrant circuit?
A.Return to the triangle of Koch, and ablate again between the posteroseptal TA and the CS ostium (region of lines #1 and #2 in Figure 16A) with improved electrode-tissue contact.
B.Return to the triangle of Koch, and ablate progressively further superior along the TA (superior to the lower dashed line in Figure 16A) until AVNRT is eliminated.
C.Terminate the procedure because there is no other safe place to ablate slow/fast AVNRT.
D.Use the resetting response to a single atrial extrastimulus at the locations of the 3 most common slow pathways (inferior triangle of Koch, roof of the CS, and left atrium [LA] close to the inferolateral mitral annulus [MA]) to identify the atrial end of the slow pathway forming the antegrade limb of this slow/fast reentrant circuit.
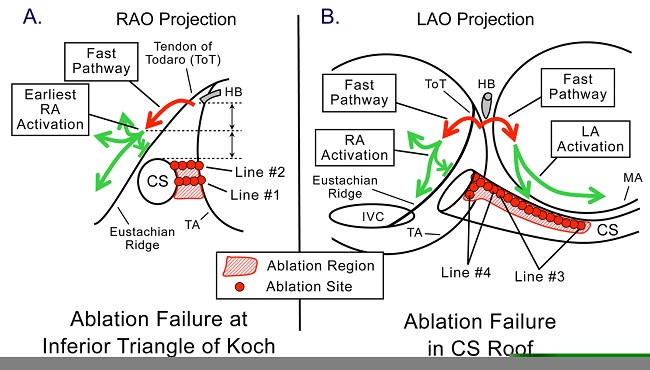
Figure 10.1. Schematic representation in the right anterior oblique (RAO) (Panel A) and left anterior oblique (LAO) (Panel B) projections of the initial pattern of right (RA) and left atrial (LA) activation during slow/fast AVNRT and the sites of ablation targeting the slow AV nodal pathway in this patient. Red arrows represent retrograde conduction over the fast AV nodal pathway. Green arrows represent the initial RA and LA activation. Earliest RA activation (Panel A) is recorded posterior to the ToT and eustachian ridge, at a height approximately halfway (middle horizontal dashed line) between the height of the site recording the most proximal HB potential (upper horizontal dashed line) and the height of the roof of the CS ostium (lower horizontal dashed line). See text for description of the ablation sites. IVC, inferior vena cava; MA, mitral annulus; TA, tricuspid annulus.
Discussion
Slow/fast AVNRT is a group of 3 tachycardias, each using the fast AV nodal pathway for retrograde conduction but differing in the slow pathway used for the antegrade limb of the reentrant circuit.1
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


