Chapter 131
Abdominal Aortic Aneurysms
Open Surgical Treatment
Edward Y. Woo, Scott M. Damrauer
Based on a chapter in the seventh edition by Brian G. Rubin and Gregorio A. Sicard
Open AAA repair is a procedure rich in history and with years of robust, long-term outcome data. Initially described in 1952 by Dubost et al, open repair has undergone continuous evolution and refinement.1 Current outcomes with elective open repair are excellent, with perioperative mortality rates between 1% and 7% depending on center volume and surgeon experience.2–4 Notably, a recent meta-analysis of the randomized trials of endovascular aneurysm repair (EVAR) demonstrated a 3.3% 30-day mortality among the combined 1342 patients repaired via the open technique.5 This is concordant with a 4% mortality reported for the highest volume centers in an administrative database study using the National Inpatient Sample (NIS),2 although single-institution case series and carefully controlled registry studies have reported even better results.3,6
Since its introduction in the early 1990s, EVAR has dramatically transformed the management of AAA. Every generation of EVAR devices has become more advanced and the indications for use (IFU) have steadily expanded to incorporate more complex anatomy.7–9 Epidemiologic studies using administrative databases attest to this, with significant reductions in the number of open aneurysm repairs performed over time in both the Medicare database10 and the NIS11; as of 2006, 60% to 70% of all AAA repairs in these populations were being performed by EVAR. Additionally, high-quality randomized controlled studies have demonstrated better short- and medium-term outcomes, and at least equivalent long-term outcomes, with EVAR, as compared with open repair.12–15 This has propelled EVAR to become the primary mode of therapy for the majority of patients with AAA, with open repair reserved for those with increasingly complex anatomy or coexisting disease process that prohibit them from an endovascular repair.16–18 Nonetheless, open AAA repair remains a mainstay of vascular surgery.
Terminology
Abdominal aortic aneurysms occur in all segments of the abdominal aorta and frequently extend into one or both common iliac arteries. The vast majority of these affect only the infrarenal aorta, allowing for proximal vascular control as well as a proximal graft anastomosis below the renal arteries. More proximal aneurysms that abut the renal arteries are considered pararenal aneurysms and can further be broken down into juxtarenal aneurysms (in which the aorta is aneurysmal just up to, but not including, the renal artery orifices) and suprarenal aneurysms (in which the aneurysmal aortic segment includes the origins of the renal arteries as well).19 Repair of juxtarenal aneurysms requires the placement of a proximal aortic cross-clamp above the level of the renal arteries, but the proximal anastomosis occurs below the renal arteries and the renal arteries themselves do not require revascularization. In contrast, repair of suprarenal aneurysms requires the placement of a proximal cross-clamp above the level of the renal arteries or often higher and requires the surgeon to specifically address the issue of renal revascularization. By definition, aneurysms that extend into the visceral segment and involve the SMA or celiac artery are considered thoracoabdominal aortic aneurysms and are categorized as Crawford type IV20; they require more extensive operations with proximal control above the celiac artery and revascularization of the visceral arteries.
Indication
Based on data from randomized trials, AAA has traditionally been recommended when the maximal cross-sectional diameter reaches 5.0 to 5.5 cm.21,22 This is due to the relative risk of mortality associated with repair comparing favorably to aneurysm rupture. In addition, rapid aneurysm growth22–24 or the presence of a symptomatic aneurysm mandates repair. In general, the decision to proceed with repair is based on balancing the risk of aneurysm rupture with the perioperative risk of repair, a calculation that has to be tailored to the individual patient based on preoperative risk factors and the risks of the proposed intervention (see Chapter 130). Accordingly, it may be prudent to observe a larger aneurysm in a high-risk patient who would need a complex open repair.
Anatomy
In the current era of endovascular therapy, open repair tends to be reserved for patients who cannot undergo EVAR. Despite the advances in device design, there remain a number of anatomic constraints that mandate open repair (Fig. 131-1).25 The proximal aortic neck is crucial to obtaining an endovascular seal and achieving technical success with EVAR; accordingly, no aortic neck or a hostile aortic neck is the leading indication for open repair.18 Proximal aortic necks that are short, angled, trapezoidal, have a high burden of thrombus, or are heavily calcified can compromise seal. In multiple studies hostile neck anatomy has been associated with graft-related complications, type I endoleaks, and early reintervention.26–28 These patients are often better served with open repairs.
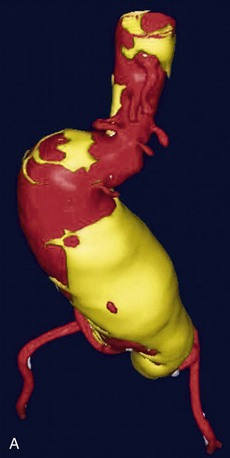
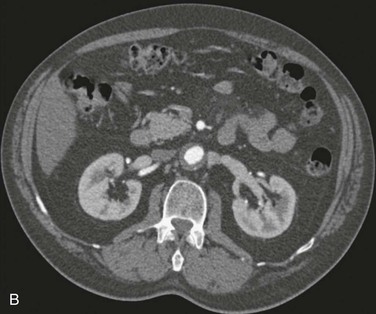
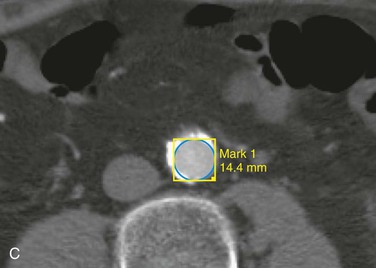
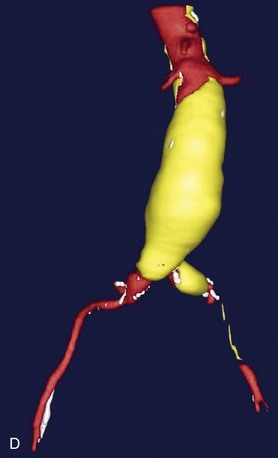
Figure 131-1 Axial images and three-dimensional CTA reconstructions demonstrating challenging aneurysm anatomy including a short, angled neck (A), circumferential thrombus (B), narrow calcified distal aorta (C), and bilateral common iliac artery aneurysms and left external iliac artery occlusion (D).
Anatomic constraints in the distal aorta and iliac arteries can also be preferentially treated with open aneurysm repair. A narrowed or calcified aortic bifurcation has been associated with limb thrombosis and EVAR failure.29 Likewise, iliac artery occlusive disease, especially chronic total occlusion, can mandate open repair for reasons pertaining to both access and treatment. Concomitant common or external iliac artery aneurysms are also indications for open repair, especially in situations in which internal iliac artery patency needs to be preserved, such as in claudicants and patients at risk for colonic, pelvic, and spinal cord ischemia.30 None of these cases is an absolute indication for open repair, especially with the introduction of newer devices such as branched endografts for the iliac arteries. However, open repair may offer the best long-term solution.
EVAR Conversion
Failure of a previous endograft due to migration or recalcitrant endoleak that is unable to be resolved via endovascular means requires open aneurysm repair. This can present at any time following EVAR. A recent meta-analysis demonstrated an average early conversion rate of 1.5% with an associated 12.4% mortality among 12,236 pooled patients, and a 1.9% late conversion rate with an associated 10% mortality among 14,289 patients.31 Despite this, single-institution case series from high volume referral centers have demonstrated superb results,32,33 with mortality rates as low as 0% among 21 patients requiring explantation.32 These interventions can be quite complex and frequently require suprarenal and supraceliac aortic control. Furthermore, the aorta and surrounding tissue can often be severely inflamed, making it quite difficult to dissect the appropriate planes. Procedural conduct of the operation is critical and understanding how to manage the endograft (full/partial removal) is important. Full discussion of aortic endograft explant is beyond the scope of this chapter. Ultimately, endograft explant is probably best reserved for centers that perform high volumes of open repair and have significant experience with explantation.
Infection
Infection of either the native aorta or of a previous open or endovascular repair requires an open operation for definitive therapy. Endovascular salvage has been described, but this would be considered more of a palliative alternative or temporary bridge to open repair.34,35 In cases of an infected prior aortic graft, excision of all prosthetic material and extra-anatomic reconstruction has long been the gold standard, but recent data suggest that the use of an aortic homograft36 or rifampin-soaked Dacron may be equally efficacious in treating the infection.37–39 However, we have found that only mycotic native aneurysms are well-treated primarily with in situ reconstructions; when treating infected aortic grafts with in situ reconstruction, reinfection has been an issue. In either situation debridement of as much infected tissue as possible is ideal in order to obtain source control. As stated earlier, EVAR or other endovascular techniques can be used but only for treatment in patients who are too high risk to undergo an open procedure; in other patients, these techniques are mainly considered temporizing measures.
Additional Circumstances
A number of special circumstances can also influence the decision to proceed with open aneurysm repair. The presence of a horseshoe kidney with multiple renal and isthmus arteries originating from the aorta and iliac arteries40 is best served with open repair so that these vessels will not be excluded.41 Likewise, patients in which the patency of the inferior mesenteric artery (IMA) needs to be maintained, such as those with bilateral hypogastric artery occlusion, SMA stenosis/occlusion, or previous colectomy, may require open aneurysm repair as well. As a counterpoint, patient factors such as a history of previous laparotomy or retroperitoneal exposure, abdominal stomas, abdominal wall defects, or poor pulmonary function, might argue for a creative endovascular approach when the patient would otherwise be best treated with an open repair.
Preoperative Assessment and Planning
Open abdominal aortic aneurysm repair is a substantial undertaking for the patient. Accordingly, appropriate attention must be paid to preoperative patient assessment and planning. Careful patient selection and preparation is critical to obtaining excellent outcomes. Because of the physiologic derangements that occur as a result of the hemodynamic stress of an aortic cross-clamp, a detailed understanding of the patient’s cardiac, pulmonary, and renal function is necessary to determine who is a candidate for open repair. Routine measurement of serum chemistries, hematologic profile, and coagulation studies is essential, as well as electrocardiogram and chest x-ray. Additionally, carotid duplex studies, transthoracic echocardiography, and pharmacologic cardiac stress testing with nuclear imaging add valuable data to help evaluate a patient’s suitability for open aneurysm repair. Some favor pulmonary function testing as well, but we have found that poor patient effort can confound the results and that careful questioning of the patient’s functional status can serve as a good estimate of pulmonary reserve. In patients with a history of significant recent weight loss, nutritional parameters may be predictive of perioperative complications. Similarly, in patients with a history of liver disease and cirrhosis, appropriately tailored preoperative studies should be considered. Other subsets of patients require special consideration, such as those with a history of cerebrovascular or Parkinson’s disease. In these individuals with diminished physiologic reserve or compromised baseline functional status, it must be determined whether the patient’s current and anticipated postoperative quality of life are sufficient to merit proceeding with an elective operation. This is especially poignant in the very elderly, in which case postoperative complications may condemn the patient to long-term skilled nursing care and permanent loss of independent functional status.
Besides patient factors, a keen understanding of an individual’s specific anatomy is necessary to adequately plan the operation and appropriately counsel the patient about the anticipated risks and benefits of the procedure. The anatomy will influence the level of the aortic cross-clamp and the complexity of the repair. Thus detailed radiographic imaging, usually in the form of contrast-enhanced computer tomography (CT) is important. These studies are necessary to understand the extent of aneurysmal, as well as occlusive, disease and to reveal any arterial or venous abnormalities that may impact the repair.
Preoperative Imaging
Since nearly all patients are evaluated for potential endovascular versus open repair, most patients selected for open repair have undergone preoperative imaging, usually by CT scanning.
Computed Tomography
Although CT angiography (CTA) with three-dimensional reconstructions, which allows for accurate anatomic measurements of a vessel’s true cross-sectional diameter and center-line length (Fig. 131-2), is invaluable for EVAR,42–45 it is also helpful for planning open repair. CTA visualizes aneurysm angulation, arterial tortuosity, arterial wall calcification, and intravascular thrombus (Fig. 131-3), which is useful for planning the best approach and clamp sites. A detailed view of the proximal aneurysm neck allows the involvement of the visceral aortic segment to be accurately determined (Fig. 131-4).46,47 From this, the need for a suprarenal or supraceliac clamp site can be made and potential clamp sites examined for the presence of heavy or circumferential calcification or thrombus. Concomitant occlusive disease of the visceral vessels and aortoiliac segment is also readily apparent on CTA, allowing decisions regarding the need for endarterectomy or complex reconstruction to be made preoperatively.48–50
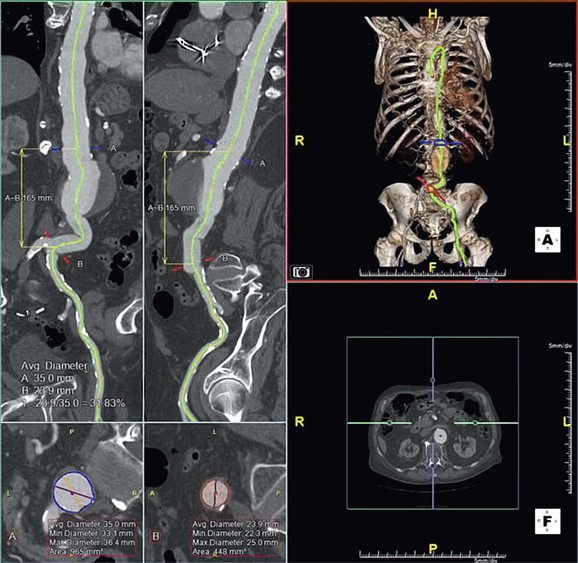
Figure 131-2 Three-dimensional CT reconstructions allow for accurate, inline measurement of aortic lengths and true cross-sectional diameter.
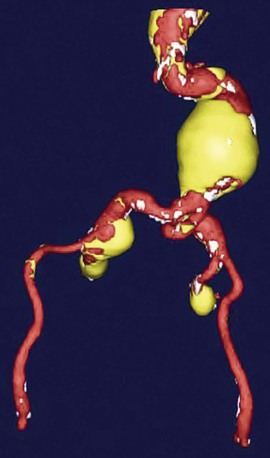
Figure 131-3 Three-dimensional CT reconstruction showing an abdominal aortic aneurysm with tortuous proximal aorta and tortuous bilateral iliac artery aneurysms.

Figure 131-4 Axial CTA image showing visceral involvement in a type IV thoracoabdominal aortic aneurysm.
CTA also provides valuable information about the venous and visceral anatomy that might alter the operative plan; the presence of a retroaortic or circumferential renal vein has implications on selecting the surgical approach and obtaining adequate exposure. Likewise, multiple renal arteries or a horseshoe kidney can affect both clamp site selection and arterial reconstruction. Appropriate visualization of the distal anatomy is also important. Concomitant stenotic, occlusive, or aneurysmal disease will influence the site of distal reconstruction, as well as the need for additional procedures. For example, additional graft limbs may be needed to preserve IMA or hypogastric flow. In addition, severe stenotic or occlusive disease can be bypassed at the time of the reconstruction.
Finally, the rate of incidental findings on CTs obtained for AAA is not inconsequential,51,52 and in certain circumstances, such as the diagnosis of an advanced malignancy, may take precedence over aneurysm repair.
Magnetic Resonance Angiography
Magnetic resonance angiography (MRA) may also be used for preoperative planning. It has been shown to be just as accurate as CT in the determination of aneurysm size and extent, as well as in the evaluation of concomitant occlusive disease.53–55 In patients with inflammatory aneurysms it may offer more information regarding the extent of the inflammatory process.56 MRA, however, does not offer information on the extent of calcification and sometimes can overestimate stenotic disease. Our preference, and that of most institutions, is to use CT.
Operative Technique
There are two widely practiced approaches to open aneurysm repair: transperitoneal and retroperitoneal. Various other methods (beyond the scope of this chapter) have been described, including minilaparotomy,57–60 laparoscopic,61–65 and robotic approaches,66–68 none of which has gained widespread acceptance.
Selecting the Approach
Because the goal of any approach is to obtain adequate exposure of the affected aortic segment, both transabdominal and retroperitoneal approaches will be technically equivalent in many situations. Under these circumstances, selection of approach should be determined by surgeon preference and familiarity.
Some situations, however, would recommend one technique over another. The transperitoneal approach offers rapid access to the infrarenal aorta with little need for complex patient positioning and is ideal for use in emergencies. In addition, for surgeons unfamiliar with the retroperitoneal approach, the transperitoneal offers a more comfortable approach to the aorta. Access to the entire peritoneal cavity also allows the surgeon to address nonvascular intra-abdominal pathology. As compared with the retroperitoneal approach, it also offers better, but not exclusive, access to the right renal artery and the right internal and external iliac arteries, as well as the femoral arteries. It is, however, more difficult to expose the visceral aortic segment from this approach.
The retroperitoneal approach, usually via a left tenth interspace incision, allows for superior exposure of the visceral and supraceliac aorta as well as the left renal artery. This is useful in managing patients with pararenal aortic aneurysms and type IV thoracoabdominal aortic aneurysms. Additionally, in patients who have undergone previous abdominal operations, it avoids the risk of “redo laparotomy” and eliminates the difficulties posed by intra-abdominal adhesions. It may also offer advantages in obese patients by allowing the abdominal contents to fall away from the surgical field.69,70 Although exposure of the right internal and external iliac artery can be more difficult from this approach, it can still be performed with appropriate careful dissection. A single-institution retrospective study of 160 open aneurysm repairs published in 2007 demonstrated that with the advent of EVAR, the rates of transperitoneal aneurysm repairs significantly declined whereas retroperitoneal repairs significantly increased, likely because of the need for more proximal aortic repairs.71 In this report, the transperitoneal approach was associated with a greater blood loss and longer suprarenal clamp times.
A number of both retrospective cohort and randomized trials have compared the outcomes of patients undergoing aneurysm repair using transperitoneal and retroperitoneal approaches. Depending on the study, retroperitoneal repair has been associated with significantly decreased postoperative fluid requirements, pulmonary edema, pneumonia, respiratory failure, postoperative ileus, shorter length of intensive care unit and overall hospital stays, shorter time to full recovery, and less costs.70,72,73 Other studies have disputed this, showing equivalency between the two procedures regarding these variables.69,74 Data regarding hernias have been mixed, with studies showing that the retroperitoneal approach is associated with more,74 equal,70 or fewer hernias and bulges.73
Transperitoneal Repair
Exposure
The patient is positioned supine on the operating table with the arms abducted, and the abdomen is prepped and draped from the nipples to the knees. A midline incision is made from the xyphoid to the pubis; if necessary, the xyphoid can be excised and the incision carried to the inferior boarder of the sternum. This allows for maximal exposure. The abdominal contents are examined for any pathology that might alter the planned procedure. The omentum and transverse colon are retracted cephalad, and the small bowel is packed in the right hemiabdomen. Adequately protected with either warm moist towels or a sterile plastic covering, both structures can be eviscerated out of the abdominal cavity to gain more working space if needed. A self-retaining retractor, such as the Bookwalter (Codman and Shurtleff, Inc., Raynham, Mass) or Omni (Omni-Tract, St. Paul, Minn) retractor, greatly facilitates exposure and should be set up at this point.
To expose the aorta, the ligament of Treitz is divided, the third and fourth portions of the duodenum are reflected to the patient’s right, and the periaortic lymphatic and connective tissue is ligated and divided (Fig. 131-5). Care must be taken to avoid injury to the inferior mesenteric vein; this structure can, however, be divided to facilitate exposure. The incision in the posterior peritoneum is then continued caudally in this plane to expose the entire infrarenal aorta. Although starting to the left of the aorta at the ligament of Treitz, the incision in the posterior peritoneum should course to the right of the aortic midline to prevent injury to the inferior mesenteric artery, sigmoid mesentery, and autonomic nervous plexus at the bifurcation. In cases in which a tube graft will be used and the distal anastomosis will be to the aorta itself, the dissection does not need to proceed beyond what is necessary to obtain distal control at the level of the bilateral proximal common iliac arteries.
Iliac Arteries
With the growth of EVAR, the relative frequency of open aneurysm repairs that involve concomitant occlusive or aneurysmal disease of the iliac arteries is increasing.17 In these instances, it can be necessary to expose the entire length of the common iliac artery, as well as the internal and external branches past the point of any pathology. One of the advantages of the transperitoneal approach is the relative ease in which the bilateral distal iliac arteries can be exposed. To do so, the posterior peritoneal incision is carried down onto the right common iliac artery, the anterior periadventitial plane of the iliac artery is identified, and the overlying tissue divided along the length of the artery to its bifurcation and beyond, as needed. The ureter overlies the bifurcation of the iliac artery in the retroperitoneum, and great care must be taken to identify, atraumatically dissect, and retract it out of the operative field. In cases of significant aneurysmal disease or inflammation, in which the ureters may be difficult to identify, preoperative ureteral stents can be highly beneficial. Division of the retroperitoneal tissues overlying the aortic bifurcation and left common iliac should be avoided to prevent damage to the autonomic nervous plexus and any associated sexual dysfunction. Rather, the cut peritoneum should be retracted toward the left to gain access to the left iliac system. If this is inadequate, a counterincision can be made in the posterior peritoneum lateral to the sigmoid colon, and the sigmoid mobilized medially to expose the bifurcation of the left common iliac artery; again, care must be taken to identify and protect the left ureter (Fig. 131-6).
Pararenal Aorta
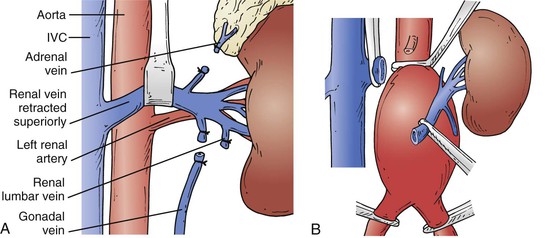
Likewise, a growing proportion of patients who require open aneurysm repairs have aneurysms with short or no infrarenal neck.16 These juxtarenal aneurysms require the placement of a suprarenal clamp, which necessitates additional proximal aortic exposure. To do so, the posterior peritoneum is opened cephalad to the level of the renal veins. Note should be made as to location of the left renal vein on the preoperative CT scan. If it is anterior, as in most cases, it can be mobilized to gain more proximal aortic exposure by dividing the gonadal, adrenal, and lumbar branches (Fig. 131-7A). Alternatively, it can be divided safely, albeit with an increased risk of postoperative renal insufficiency.75–77 The decision to divide the left renal vein needs to be made before it is aggressively mobilized, because once it is divided, the gonadal, adrenal, and lumbar branches must be preserved in order to maintain adequate venous drainage; to facilitate this and maximize exposure, this should be done as close to the inferior vena cava as possible (Fig. 131-7B). If a retroaortic or circumferential left renal vein is present, care must be taken during placement of the proximal clamp because the tips of the clamp can injure the vein.
Supraceliac Aorta
The supraceliac aorta is exposed by dividing the lesser omentum or gastrohepatic ligament. The aorta is identified by palpation, and the overlying fibers of the right crus of the diaphragm are divided with electrocautery. Mobilization of the left lobe of the liver by dividing the left triangular and coronary ligaments, as well as the falciform ligament, can assist with exposure but is often not necessary. Additionally, the presence of a nasogastric tube helps to identify the esophagus and thereby protect it from inadvertent injury. The esophagus is typically retracted to the left. The aorta can be dissected anteriorly down to the level of the celiac axis, although care must be taken to avoid injury to the pancreas as one proceeds caudally.
Medial Visceral Rotation.
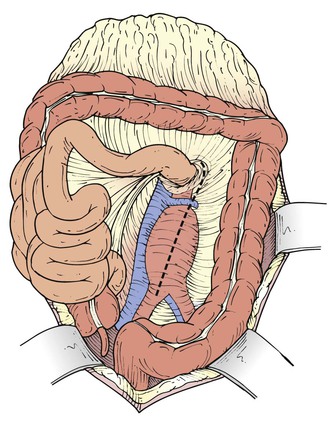
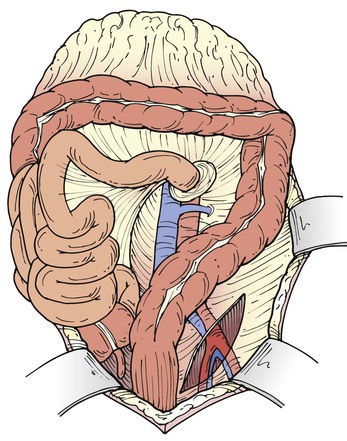
Suprarenal aneurysms are best approached using a retroperitoneal exposure. Despite this, the complete visceral segment of the aorta can be accessed transperitoneally using a left medial visceral rotation (Fig. 131-8). The left colon is mobilized by incising the posterior peritoneum just lateral to the line of Toldt. This incision is then carried cephalad through the phrenicocolic ligament and then medially toward the aortic hiatus along the underside of the diaphragm. The plane separating the posterior aspect of Gerota’s fascial and posterior abdominal wall is developed, allowing the colon, pancreas, spleen, and left kidney to be reflected medially. As the kidney is mobilized, the left renal lumbar vein should be identified and ligated to prevent avulsion. Alternatively, the kidney can be left in the renal fossa; this requires dividing the linorenal and linophrenic ligaments and developing a plane between the anterior surface of Gerota’s fascia and the posterior surface of the colonic mesentery and pancreas (Fig. 131-8C).
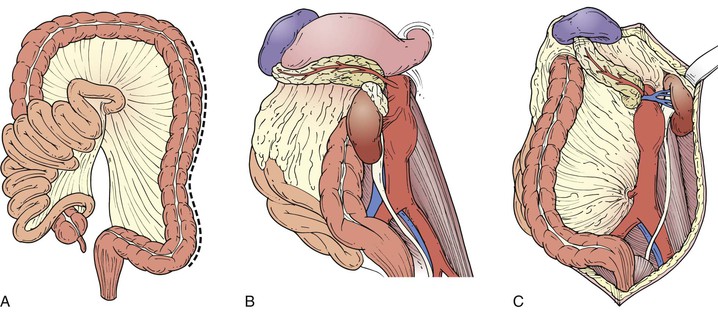
Figure 131-8 When using the transperitoneal approach, a left medial visceral rotation facilitates access to the visceral segment of the aorta. The peritoneum is incised along the line of Toldt (A) and the left colon, pancreas, and spleen are mobilized medially. The kidney can be mobilized en bloc (B) or left in the renal fossa (C).
Arterial Reconstruction
Once the appropriate aortic segments are exposed, the proximal and distal clamp sites are identified. Encircling the vessels with silastic vessel loops or cloth umbilical tape is not necessary and increases the risk of injury to posterior structures, especially the iliac veins. Only enough exposure to apply a clamp is needed. Care must be taken to avoid injuring or avulsing closely related venous structures. The patient is systemically heparinized, and the aorta and iliac arteries are clamped. Distal clamps are usually applied first to prevent any thrombus from embolizing to the legs during application of the proximal clamp. The aneurysm is opened via a longitudinal aortotomy, which transitions to a T-shaped incision at the proximal and distal ends to allow for the graft anastomosis (Fig. 131-9). The proximal anastomotic site is cleared of thrombus and calcium, and an end-to-end anastomosis is performed using a running polypropylene suture. A discussion of more complex proximal anastomoses for suprarenal and type IV thoracoabdominal aortic aneurysms can be found later in the section on retroperitoneal repair. The use of aortic retention sutures or a self-retaining retractor placed in the aneurysm sac helps to facilitate exposure. Thrombus is then cleared from the remainder of the aneurysm sac and back-bleeding lumbar vessels are controlled; management of the inferior mesenteric artery is discussed in its own section later in this chapter. The distal reconstruction is performed in a similar fashion (Fig. 131-10) allowing for forward flushing of the graft and back bleeding of the distal vessel before completing the anastomosis.
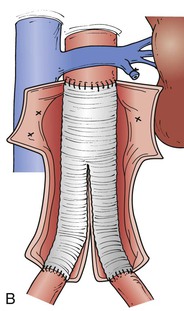
Closure
After hemostasis has been obtained, the aneurysm sac is closed over the graft using a running absorbable suture. The posterior peritoneum is likewise closed (Fig. 131-11). Both of these maneuvers help to exclude the bowel from the retroperitoneal and prevent contact between the bowel and the graft. If the sac or retroperitoneum is unable to be approximated over the graft, the omentum can be brought down to cover the graft. It is critical to obtain separation of the graft from the bowels to prevent future aortoenteric fistulization. The intestines are then returned to their normal anatomic position, and the anterior abdominal wall closed according to surgeon preference.
Retroperitoneal Repair
Exposure
The patient is placed in right lateral decubitus position with the break in the table centered at the iliac crest. The table is maximally flexed and then leveled. A surgical beanbag positioner is used to help secure the patient in this position. Care must be taken to appropriately pad and protect the right axilla. The chest and abdomen and left groin are prepped and draped in the standard fashion. Access to the right groin can be obtained, if needed, by flexing the hips posteriorly
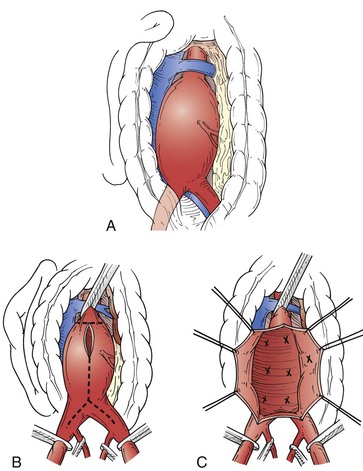
The incision starts in the 10th intercostal space at the posterior axillary line; this can be varied depending on the proximal extent of the aneurysm (Fig. 131-12). It is carried onto the abdomen, where it runs lateral and parallel to the lateral boarder of the left rectus muscle and terminates below the umbilicus at a level determined by the distal extent of the intended arterial reconstruction. The skin and subcutaneous tissues are divided to expose the anterior fascia of the external oblique. The external oblique, internal oblique, and transversus abdominis muscles are sequentially opened over a short distance using a combination of blunt dissection and electrocautery. Care must be taken not to violate the peritoneum. The peritoneum is then blindly freed from the abdominal wall and diaphragm using careful blunt digital dissection. This permits the abdominal cavity to be opened to the level of the diaphragm. Exposure can be increased by entering the chest through the 10th intercostal space contiguous with the abdominal portion of the incision by dividing 2 to 3 centimeters of the diaphragm. The left psoas muscle is identified, and the peritoneal and retroperitoneal contents are swept anteriomedially throughout the length of the wound, as well as off the inferior surface of the diaphragm. This exposes the entire intra-abdominal aorta (Fig 131-13A). At this stage, the left ureter should be identified and protected, because it runs anterior to the aorta and left common iliac artery. By staying on a plane directly anterior to the iliac arteries, the right ureter can also be identified and protected. A Bookwalter or Omni retractor can now be put in place to assist with exposure. If the patient has a posterior left renal vein, it may be advisable to not mobilize the kidney during the aortic exposure and to leave it in place in the retroperitoneum. Alternatively, it can be divided for exposure as long as the gonadal branch is preserved.
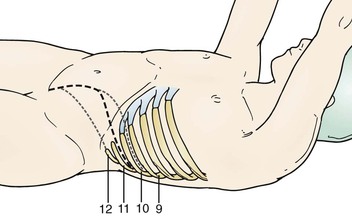
Figure 131-12 Incision (heavy line) for retroperitoneal aortic exposure. Alternate incisions are shown in gray.
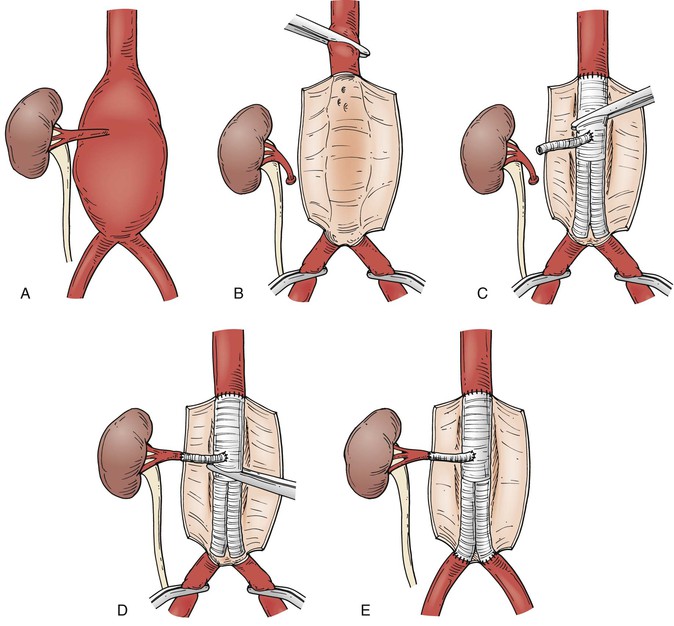
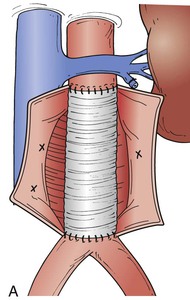
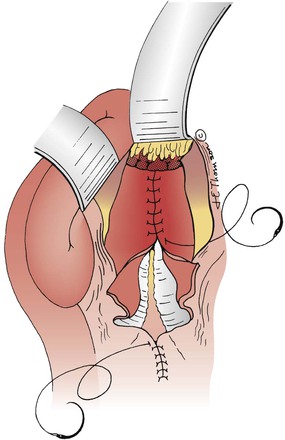
Figure 131-13 Beveled anastomosis with left renal bypass for a type IV thoracoabdominal aortic aneurysm. The aorta is clamped and opened with a T-shaped incision and the left renal artery is detched (A, B). The proximal anastomosis is beveled into the visceral segment and right renal artery, and the clamp is then advanced distal to the anastomosis (C). The left renal aretery is bypassed with a presewn side arm from the graft (D). The distal anastomoses are completed and the clamp removed (E).
Iliac Arteries
The left common iliac artery is easily identified at the aortic bifurcation and can be dissected out along its length in a rather straightforward fashion. This allows for clamp placement and reconstruction at multiple levels. Control of the proximal left internal and external iliac arteries can likewise be rather easily achieved. The right iliac artery system can be exposed by continuing to mobilize the peritoneal sac off of the retroperitoneum past the midline in the inferior wound. Depending on the patient’s body habitus, it can be challenging to expose the right internal and external iliac artery and intraluminal balloon occlusion may have to be used for vascular control after opening the aneurysm sac.
Supraceliac Aorta
To gain better access to the visceral segment of the aorta and obtain a supraceliac clamp site, the left crus of the diaphragm is divided. A suitable spot for clamping is identified and the aorta is bluntly dissected along its anterior and posterior surfaces; care must be taken to avoid avulsing any lumbar arteries or veins that run posteriorly. Again, it is unnecessary to attempt to fully encircle the aorta or iliacs; this risks esophageal, caval, or iliac vein injury. The left renal artery is identified and dissected back to its origin so that it is not injured during the opening of the aorta. Lumbar branches of the left renal vein are also identified, ligated, and divided to prevent avulsion.
Arterial Reconstruction
The use of a retroperitoneal incision is ideal for reconstruction of suprarenal and type IV thoracoabdominal aortic aneurysms given the exposure it provides. After heparinization and supraceliac cross-clamping, the aneurysm is opened with a longitudinal aortotomy up to the level of normal proximal aorta, whereupon the aortotomy is transitioned into a T-shaped incision; it is important to have previously identified the origin of the left renal artery and to have divided the renal lumbar veins to avoid injuring these structures during this maneuver (Fig. 131-13B). The left renal artery is freed from the aortic wall with a small cuff of surrounding aorta and retracted out of the immediate field.
Once the proximal extent of the aneurysm has been opened, the celiac, SMA, and right renal arteries are identified from the inside the aorta. Any significant stenosis detected on preoperative CTA, or at the time of operation, can be treated with either endarterectomy or a balloon-mounted stent deployed through the open aorta.78 The proximal extent of the graft is beveled to incorporate the celiac, SMA, and right renal arteries, and the proximal anastomosis is completed using a running polypropylene suture (Fig. 131-13C). The proximal graft is clamped, and the supraceliac cross-clamp is removed to allow perfusion of the viscera and right kidney (Fig. 131-13D). The left kidney is now revascularized by bypass with a sidearm from the graft. If a bypass is to be performed, a hybrid stent graft can be fashioned as a sidearm from the main graft before aortic cross-clamping in order to reduce left renal ischemia time and to facilitate the anastomosis (Fig. 131-14). Once the anastomosis to the left renal artery is complete, the aortic cross-clamp can be shifted distally on the graft to allow for complete renal perfusion (Fig. 131-13E). Minimizing ischemic time to this area is paramount; thus proper conduct of the operation and attention to technique is critical.
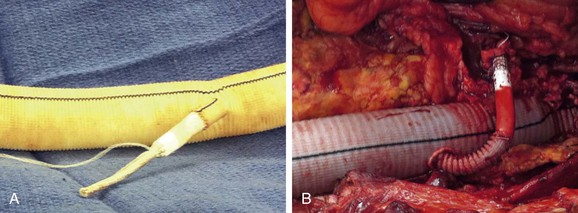
Figure 131-14 The left renal artery is revascularizated with a hybrid stent graft sewn to sidearm from the aortic graft. Before (A) and after (B) graft anastomoses are performed.
At this point the aneurysm sac is cleared of thrombus, and back-bleeding lumbar arteries are oversewn. By leaving the thrombus in situ until this point, visceral and renal ischemic time is reduced, because time is not wasted controlling bleeding with a supraceliac clamp in place. Moreover, the thrombus acts to obstruct the back-bleeding vessels and minimize blood loss. Distal reconstruction proceeds in a manner similar to that of the transabdominal approach.
Closure
After obtaining hemostasis, the self-retaining retractor system is removed and the peritoneal sac returned to its normal anatomic configuration. Because the peritoneum has not been violated, the graft remains separate from the peritoneal contents and the aneurysm sac does not need to be closed at the conclusion of the repair. Any rents in the peritoneum, however, should be closed; this can be accomplished with running absorbable suture. The flex is taken out of the operating table to remove tension on the wound during closure and the flank incision is closed in multiple layers. The ribs and diaphragm can be incorporated into the closure of the transversus abdominis and internal oblique muscles in a single layer of running absorbable suture. Great care must be taken to avoid inadvertent colonic injury during closure because the consequence of this would be disastrous. The external oblique, with its associated fascia, is closed over this in an interrupted manner because it provides the strength for the closure.
Anatomic Considerations
A number of anatomic situations exist that can complicate open aneurysm repair and require additional planning to address. Fortunately, the vast majority of these should be detected on the preoperative CTA and plans can be made to address them in a proactive manner.
Management of the Inferior Mesenteric Artery
Note should be made on the preoperative CTA as to the patency of the IMA. If it is thrombosed, then it is of no further consideration. On the contrary, if there is significant SMA disease, bilateral hypogastric artery occlusions, a large IMA, or prior colectomy, IMA preservation may be indicated. However, IMA management should not be guided by imaging alone. At the time of operation, brisk back-bleeding from the IMA suggests that it can be safely ligated, whereas sluggish or no back-bleeding from an IMA that is known to be patent, or evidence of colonic ischemia, argues for revascularization. This can be accomplished either by reimplantation of the IMA into the graft using a small cuff of surrounding aorta or in an end-to-end fashion from a sidearm attached to the body of the graft. This is easily performed from both the transperitoneal and retroperitoneal approaches.
Renal Abnormalities
The presence of renal anomalies, such as a horseshoe kidney, pancake kidney, and crossed-fused renal ectopia, complicates open aneurysm repair. Such abnormalities are most frequently associated with aberrant or multiple renal arties.79–84 Furthermore, accessory renal arteries originating from the iliac arteries or aneurysm sac are not uncommon.83 Almost all of these findings are evident on preoperative CTA; thus they should not come as a surprise at the time of operation. Many of these arteries are small and only detectable on fine-cut CTA. Thus renal abnormalities should alert one to the need for a fine cut CTA rather than standard CT. Their identification also may merit additional investigation to interrogate the anatomy of the collecting system and ureters in order to detect any associated abnormality or aberrancy; this frequently involves the use of urography.79,81,84 A renal perfusion scan can also be of assistance in this setting in helping to determine the functionality and contribution of not only each kidney but each portion of the respective kidneys. This is then helpful to determine what, if any, tissue can be sacrificed. Management is difficult because these situations pose technical challenges with respect to both exposure and revascularization, and longer aortic cross-clamp times have been reported.82 It is generally recommended that all important accessory renal arties be reimplanted; this can be done with branch grafts or through use of a Coselli’s patch. Both transperitoneal81,84 and retroperitoneal80,82,83 approaches offer options with regard to exposure, vascular control, and reimplantation. If multiple critical arteries need to be reimplanted, necessitating longer ischemic times, the use of extracorporeal perfusion strategies may be helpful to minimize kidney injury.
Venous Abnormalities
Based on surgical and radiological studies, significant venous abnormalities of the renal veins and IVC are present in between 1% and 10% of the population respectively.85–88 The most common abnormalities include retroaortic left renal vein, circumaortic left renal vein, left-sided IVC, and duplicated IVC; accessory left renal veins and preaortic confluence of the iliac veins have also been described. These abnormalities can pose significant challenges with regard to aortic exposure and can complicate the operation.88–90
With a circumaortic or retroaortic left renal vein, the posterior component can be disrupted when obtaining control of the aorta during a transperitoneal approach. In cases of a retroperitoneal approach, altering the exposure to leave the kidney in the renal fossa can assist in exposing the aorta. It is important to note that a retroaortic left renal vein can enter the vena cava either in an orthotopic position or at the more caudal L4 to L5 spinal level with the gonadal and ascending lumbar veins. Ultimately, dividing the left renal vein is acceptable as long as the gonadal and other collateral vessels are preserved.
CT scan is effective at diagnosing these abnormalities and determining their exact anatomic location. Failure to appreciate them on preoperative imaging can result in catastrophic hemorrhage,90–92 and formulating a strategy to managing these abnormalities before the operation is important. Even when a CT has been obtained, great diligence is warranted; the absence of expected normal venous anatomy should alter the surgeon to the possibility of aberrant venous anatomy.
Coexisting Pathology
When an aneurysm and other pathology are concomitantly diagnosed, the one that is more life threatening should be addressed first. Additional studies may be necessary to fully define the extent of the nonaortic pathology because the results may impact the decision to proceed with aneurysm repair. Although it has been successfully described in limited series,93,94 simultaneous operations, especially those that include the gastrointestinal tract, are to be avoided in order to prevent infection of the prosthetic graft. An exception can be made for clean procedures, such as renal resection.95,96 However, the overall clinical status of the patient has to be taken into account. A better approach may be closely staging the procedures,97 because an increased incidence of aneurysm rupture has been reported following unrelated laparotomy.98–101 The ability to do this has been greatly advanced by the advent of minimally invasive surgical techniques for gastrointestinal and genitourinary tract pathology, limiting recovery following these procedures and allowing the aneurysm repair to proceed without significant delay. Alternatively, the best approach may be treating the aneurysm with an endovascular aneurysm repair in order to facilitate a more rapid recovery and to prevent violation of the peritoneum or retroperitoneum.102 In the rare instance that coexisting pathology is found intraoperatively, the aneurysm repair should proceed as planned unless the secondary pathology is so severe as to directly impact the patient’s immediate life expectancy or poses significant risk of graft infection.
A special mention should be made of cholelithiasis. Gallstones are more prevalent in patients with abdominal aortic aneurysms.103 Despite this, the rate of acute cholecystitis in the early postoperative period is low.104–106 Simultaneous open aneurysm repair and cholecystectomy have been reported using either a transperitoneal approach or a combination of retroperitoneal abdominal aortic aneurysm repair and laparoscopic cholecystectomy.106–109 Although simultaneous aneurysm repair and cholecystectomy have been shown to be safe, it is generally not necessary and not worth the risk of graft infection.105 In the rare case of postoperative acute cholecystitis, a percutaneous cholecystostomy tube can be used to temporize the situation until the patient has recovered from the aneurysm repair.
Intraoperative Management
Open aortic surgery is a high-risk endeavor in a high-risk patient population. Precise management of the patient’s intraoperative physiology is essential to achieving good outcomes. Although operative management of the vascular surgery patient is discussed elsewhere, the pathophysiologic responses to aortic cross-clamping and the ensuing organ ischemia distinguish open aortic surgery from other vascular interventions. This topic is especially important because the increased complexity of open aneurysms results in a greater percentage of patients requiring more proximal aortic cross-clamping. Although an infrarenal aortic cross-clamp is well tolerated in most patients, supraceliac clamping produces profound alterations in splanchnic and renal blood flow and significant associated physiologic derangement.
Cardiac Function
The application and removal of an aortic cross-clamp results in a complex series of physiologic derangements governed primarily by the level at which the aorta is clamped.110,111
Aortic Clamping
As the aortic clamp is applied, systemic vascular resistance increases because of the impendence of flow. In the setting of an infrarenal aortic clamp, this can result in up to a 10% increase in arterial blood pressure with little or no change in heart rate. As distal flow is interrupted, blood volume is shifted to the central circulation and more proximal organs. If the clamp is located in the infraceliac aorta, blood flow is redistributed to the splanchnic circulation, which correspondingly augments its venous capacitance; this results in little to no change in cardiac preload. When the clamp is placed above the celiac artery, however, the splanchnic circulation cannot act as a reservoir and cardiac preload increases dramatically as the extra blood volume is shifted predominantly to the central circulation.
The combined increase in afterload and preload result in increased cardiac contractility and myocardial oxygen demand. In individuals with no left-ventricular dysfunction and no ischemic heart disease, this is well tolerated because of cardiac autoregulation. If the myocardium is not able to respond to the increased demands by augmenting contractility, or the coronary vasculature prohibits augmentation of increased blood flow, end-systolic and end-diastolic pressure and volume increase, ejection fraction decreases, and subsequent loss of cardiac output occurs. A study assessing cardiac performance in patients undergoing aneurysm repair demonstrated that infrarenal cross-clamping resulted in only minimal changes in blood pressure, filling pressure and volume, ejection fraction, and left ventricular wall motion, whereas supraceliac cross-clamping produced a 50% increase in mean arterial blood pressure, 40% increase in filling pressures, 28% increase in end-diastolic and 70% increase in end-systolic volume, and 40% decrease in ejection fraction. Although there was no evidence of left ventricular wall motion abnormalities associated with infrarenal aortic cross-clamping, they were present in 33% of patients with suprarenal and 92% of patients with supraceliac cross-clamps.112
Aortic Declamping
Removal of the aortic cross-clamp is associated with dramatic drops in arterial blood pressure. Unclamping results in a significant and instantaneous reduction in peripheral vascular resistance. As blood pools in the formerly ischemic tissues as a result of reperfusion hyperemia, central hypovolemia develops, further exacerbating hypotension. Toxic metabolites, lactic acid, reactive oxygen species, and prostaglandins accumulate in the ischemic tissue during the aortic cross-clamp and their release into the circulation promotes vasodilation and myocardial depression. Utilizing the most distal cross-clamp site possible, minimizing clamp time, and volume loading before unclamping can all help to prevent the ensuing hypotension. In extreme cases vasoactive medications may be used to assist with blood pressure augmentation, or the cross clamp may need to be temporarily reapplied. However, both of these maneuvers are less desirable because perfusion is limited.
Management
The dramatic effect of aortic cross-clamping on the patient’s physiology must be managed in real time by the anesthesia team. Effort must be directed at maintaining adequate blood pressure and perfusion while avoiding excessive hypertension. Care must be taken to optimize preload and afterload to minimize the effects of cross-clamping on myocardial oxygen demand. Mean arterial pressure must also be reduced before application of the cross-clamp. This must all be done in a way that anticipates the ultimate need to remove the aortic cross-clamp and the ensuing hypotension. Accordingly, clear and direct communication between the surgeon and anesthesiologist is crucial around the time of the application and removal of the cross-clamp, so that the physiology can be managed appropriately. We typically give the anesthesiologist a prediction of the approximate duration of cross-clamping before beginning and then provide a several-minute warning before removal. A dedicated anesthesia team for these procedures likely results in the best outcomes.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


