Zenker’s Diverticulum and Diverticulopexy
Presentation
A 65-year-old man with no significant past medical history presents to your office with symptoms of dysphagia and regurgitation. He reports difficulty initiating swallowing both solids and liquids. He also experiences occasional spontaneous regurgitation of undigested food into the back of his throat. There is no history of cough or pneumonia. His wife reports that in recent months she noticed that her husband has bad breath. He has had no weight loss, and his physical examination is normal.
Differential Diagnosis
The differential diagnosis for dysphagia includes malignant obstruction, benign stricture, leiomyoma, extrinsic compression, motility disorder, diverticulum, disorders of the nervous system producing discoordinated swallowing, and congenital abnormalities of the esophagus such as duplication cyst. The history in this patient of difficulty initiating swallowing suggests a disorder of the cervical esophagus or a nervous system disease.
Recommendation
Options for initial investigation include endoscopy or a contrast x-ray of the esophagus and stomach. In this case, because the most likely diagnoses include a motility disorder, a contrast esophagram is the best initial test. If the patient has an unexpected diverticulum, there is an increased risk for perforation during an initial endoscopic examination.
▪ Esophagogram
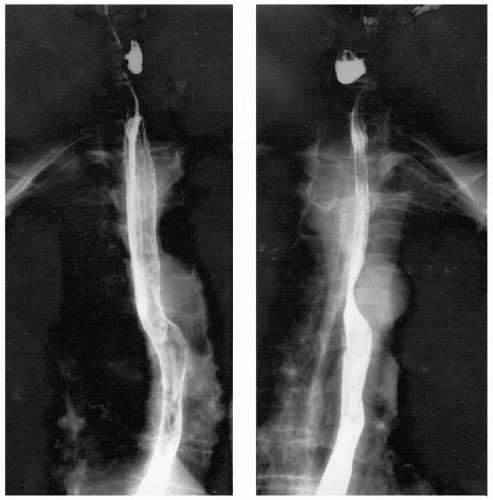 Figure 9-1 |
Esophagogram Report
The barium swallow demonstrates a mild nonspecific motility disorder of the esophageal body, a small hiatal hernia, and a pharyngoesophageal diverticulum.
Discussion
A pharyngoesophageal, or Zenker’s, diverticulum usually occurs in patients older than 50 years of age, and results from discoordination between the inferior pharyngeal constrictors and the cricopharyngeus muscle. In some patients, the only manifestation of this discoordination is the presence of a poorly relaxing cricopharyngeus muscle (cricopharyngeal bar) that impinges on the hypopharyngeal lumen. Long-standing excess pressure ultimately causes the development of a diverticulum in the region between the two muscles that has a paucity of overlying muscle, known as Killian’s triangle. These diverticula can become quite large, extending into the mediastinum.
Patients with pharyngoesophageal diverticula are at risk for regurgitation and aspiration, particularly if the diverticulum is large. In patients with symptoms, correction of the abnormality is recommended. Endos copy and manometry are not necessary components of the preoperative evaluation because they rarely have an impact on the management of this diagnosis.
The main therapeutic objective is the interruption of discoordinated activity between the inferior pharyngeal constrictor muscle and the cricopharyngeus muscle. This is accomplished by division of the cricopharyngeus muscle (myotomy). Management of the diverticulum may include excision or plication to the prevertebral fascia in an inverted orientation. For diverticula that are moderate in size (2 to 4 cm in length), endoscopic management may be considered. A
linear cutting stapler is placed transorally, with the staple cartridge in the esophagus and the anvil in the diverticulum. Firing the stapler divides the cricopharyngeus and creates a common cavity between the esophagus and the diverticulum. This procedure is not recommended for very small or very large diverticula.
linear cutting stapler is placed transorally, with the staple cartridge in the esophagus and the anvil in the diverticulum. Firing the stapler divides the cricopharyngeus and creates a common cavity between the esophagus and the diverticulum. This procedure is not recommended for very small or very large diverticula.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


