Wound and Lymphatic Complications Following Lower-extremity Revascularization
Christopher M. Alessi
Robert M. Zwolak
A broad range of wound and lymphatic complications may follow infrainguinal arterial reconstruction, some of which are potentially catastrophic (Table 54-1). The more common problems include superficial wound infection, skin edge necrosis, small wound hematoma, seroma, and self-limited lymph leak. These issues are easily treated and not typically associated with significant morbidity. Much less common but vastly more complex are persistent lymphocutaneous fistula, pseudoaneurysm formation, graft infection, and anastomotic disruption. Due to this wide range of severity, the reported overall incidence of wound complications following infrainguinal bypass surgery, 7% to 44%, is not very meaningful. As an example of a larger reported series, Wengrovitz et al. retrospectively analyzed 163 subcutaneous autogenous lower-extremity vein bypass grafts and found wound complications in 28 (17%). Just over half of these (57%) were infections confined to the dermis or extending into the subcutaneous fat, not exposing or involving the bypass conduit. These were all treated successfully with bedrest, parenteral antibiotics, and local wound care, which included bedside debridement and dressing changes. Twelve patients (43%) had deeper wound complications leading to exposed or infected grafts. They were treated with operative debridement and soft tissue coverage. Of these, four patients (2.5% of the series) required major amputation; one of these patients later died.
Predisposing Factors
Many groups have tried to identify factors that increase the likelihood of developing a wound infection. Advanced age, obesity, diabetes mellitus, renal failure, anemia, steroid therapy, ipsilateral limb ulceration, and severity of ischemia have all been analyzed. In the series note above, Wengrovitz et al. identified two medical conditions and two technique-related variables holding a statistical association with wound infections. These conditions were presence of an ipsilateral limb ulcer, chronic steroid use, bypass to the dorsalis pedis artery, and use of saphenous vein in situ technique. Schwartz et al. also found a significant association between wound complications and the procedure-related variables of a continuous incision used for in situ bypass and bypass to the anterior tibial artery. They found no association with age, sex, hypertension, smoking, diabetes, indication for surgery, mean ankle-brachial index, method of wound closure, or the duration of surgery. Kent et al. found no significant predictors of wound complications using a univariate analysis, but advanced age and obesity increased the chance of wound complications when analyzed with multivariate methodology. Consistent with others, they found no association with diabetes or renal failure.
Wound Hematomas and Seromas
Wound hematomas and seromas can adversely affect wound healing by causing skin edge separation and providing a nidus for infection. Good surgical technique and meticulous hemostasis should be obtained before wound closure. Closed-suction drainage should be considered in situations where post-closure bleeding is likely, e.g., patients requiring immediate postoperative anticoagulation, those leaving the operating room anticoagulated, and those taking clopidogrel or ticlopidine. Large hematomas or seromas that develop and are symptomatic (e.g., severe pain, threatened overlying skin, falling hematocrit) should be drained in the operating room where the wound can be fully evaluated and appropriate equipment and personnel are available to deal with potentially significant hemorrhage and the need for a more involved procedure.
Pseudoaneurysms
Pseudoaneurysms usually develop at an anastomosis and are more likely to develop in the setting of an infection. The femoral region is the most common site, and occurrence is statistically greater with prosthetic material than with vein conduit. Repair is usually accomplished with direct autogenous or a prosthetic interposition graft if the site is not overtly infected. Infection may be present even when the site does not
demonstrate typical findings, such as inflammatory change or purulence. Occult infection has been documented post-hoc in up to 60% of femoral pseudoaneurysms that were repaired in the absence of overt infection.
demonstrate typical findings, such as inflammatory change or purulence. Occult infection has been documented post-hoc in up to 60% of femoral pseudoaneurysms that were repaired in the absence of overt infection.
Table 54-1 Wound Complications Following Lower-extremity Revascularization | |||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
|
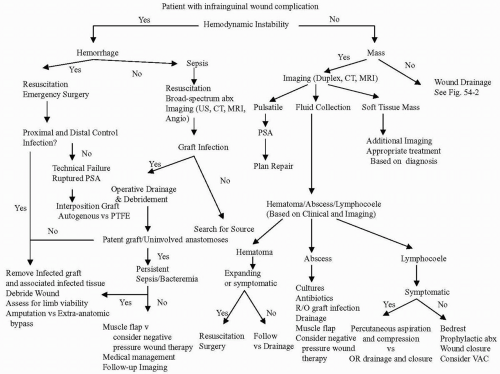 Figure 54-1. Algorithm for approaching infrainguinal wound complications. Adapted from Calligaro. |
Exposed Grafts
Exposed grafts, especially those with exposed anastomoses, are vulnerable to graft breakdown leading to life-threatening hemorrhage. Both polytetrafluoroethylene polytetrafluoroethylene (PTFE) and autogenous vein reconstructions are at risk, and it is not entirely clear which of the two conduit types is associated with the worst patient outcomes in this situation.
A major step in dealing with exposed conduit is soft tissue coverage. Wengrovitz et al. used sartorius flaps, while others accomplish coverage with gracilis, rectus abdominis, and rectus femoris muscle flaps, or even pedicle omental flaps. Maser et al. reported a series of 14 patients with 15 exposed, eroded, or infected prosthetic vascular grafts in the groin, all of which healed with sartorius muscle flaps. Schutzer et al. recently described their experience with sartorius muscle flaps in 50 patients. The grafts were split evenly between native vein and prosthetic material. They performed wide debridement and graft coverage with sartorius muscle flap. There was an 8% major amputation rate and a 12% 30-day mortality rate. One patient developed a late pseudoaneurysm that was removed. None of the procedures has resulted in further systemic or graft sepsis, and there were no arterial or graft blowouts over an average 18-month follow up. They concluded that closure of groin and thigh wounds with exposed bypass graft or native artery can be safely performed with the sartorius muscle flap with excellent results. Likewise, Morasch et al. describe 18 patients with nonhealing and infected groin wounds that were treated with pedicled gracilis muscle flaps. These series are sufficiently individualized to make it difficult to determine which of these choices may be clinically superior.
Newer strategies for managing infected vascular grafts in the groin include the use of negative-pressure vacuum-assisted wound care (VAC). Demaria et al. report a case of an elderly diabetic woman with a groin infection after a femoropopliteal bypass using reversed greater saphenous vein. On postoperative day 14 her wound was debrided, leaving exposed vein conduit. A VAC was applied, and the wound healed without complication. Vascular surgeons at our




Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
