Wheezing
Jud W. Gurney, MD, FACR
DIFFERENTIAL DIAGNOSIS
Common
Asthma
Cardiogenic Pulmonary Edema
Pulmonary Emboli
Aspiration
Less Common
Airway Obstruction
Extrinsic: Airway Compression
Intrinsic: Airway Narrowing
Allergic Bronchopulmonary Aspergillosis
Tracheobronchomalacia
Churg-Strauss Syndrome
Eosinophilic Pneumonia
Rare but Important
Carcinoid
Diffuse Neuroendocrine Hyperplasia
Mastocytosis
ESSENTIAL INFORMATION
Key Differential Diagnosis Issues
Wheezing: High-pitched adventitious sound superimposed on normal sounds of breathing; occurs when air flows rapidly through narrowed bronchi
Helpful Clues for Common Diagnoses
Asthma
“All that wheezes is not asthma”
Primarily involves small to medium-sized bronchi
Bronchial wall (BW) thickened by edema, ↑ smooth muscle, ↑ size mucus glands
HRCT: BW thickening in 50-90%
Near-fatal asthma: Centrilobular nodules ↑, (seen in 100%) but not specific (seen in up to 1/3 of mild asthma)
Air-trapping (total volume > 1 segment) in 50%
Complications of asthmatic attacks
Pneumomediastinum (5%)
Pneumonia (2%)
Pneumothorax (0.3%)
Lobar atelectasis from mucus plugs (rare)
Cardiogenic Pulmonary Edema
Interstitial edema thickens bronchial walls, narrowing their lumen
Associated findings: Cardiomegaly, pleural effusions, interstitial septal thickening
Pulmonary Emboli
Acute emboli associated with reflex bronchoconstriction of embolized segment, leads to wheezing
Recurrent emboli may give rise to episodic wheezing and misdiagnosis of asthma
10% of patients with acute pulmonary emboli have wheezing as predominant symptom
Aspiration
Repeated episodes of aspiration may give rise to wheezing as aspirated material narrows airway lumen
Aspiration most common in dependent segments
Posterior segments of upper lobes and superior segments of lower lobes in recumbent position
Lower lobe basilar segments in upright position
Helpful Clues for Less Common Diagnoses
Airway Obstruction
Extrinsic: Airway Compression
Most commonly goiters, vascular rings
Intrinsic: Airway Narrowing
Most commonly from neoplastic and nonneoplastic tumors, tuberculosis, or foreign bodies
Even with fixed obstruction, patient may have intermittent wheezing and be misdiagnosed with asthma for mths or yrs
Allergic Bronchopulmonary Aspergillosis
Hypersensitivity reaction to Aspergillus fumigatus
Occurs in 1-2% of chronic asthmatics
HRCT: Central bronchiectasis with peripheral sparing, primarily involves upper lung zones
Tracheobronchomalacia
Softening of airway cartilage
Excessive collapse (> 70%) of expected luminal area during expiratory CT scan
Typical morphology: Crescent, lunate, or “frown” sign
Churg-Strauss Syndrome
Granulomatous small vessel vasculitis
Most present with peripheral neuropathy (mononeuritis multiplex)
Nearly 100% have asthma
Triad of allergic history, peripheral blood eosinophilia, and systemic vasculitis
CT: Nonspecific but similar to chronic eosinophilic pneumonia with peripheral consolidation and ground-glass opacities
Pleural effusions in 25% (extremely rare in eosinophilic pneumonia)
Eosinophilic Pneumonia
Asthma seen in 50% of chronic eosinophilic pneumonia
Striking peripheral consolidation, primarily of upper lung zones
Helpful Clues for Rare Diagnoses
Carcinoid
Carcinoid syndrome: Wheezing from excess serotonin and histamine
Carcinoid syndrome uncommon with pulmonary carcinoids, seen in 2-5% of patients, almost all of whom have hepatic metastases
Endobronchial component of carcinoid tumors may give rise to unilateral wheezing
Hemoptysis also common as tumors are vascular
Diffuse Neuroendocrine Hyperplasia
Rare disorder of proliferation of carcinoid tumorlets (benign)
Primarily women; may also be more common in those living at high altitude
Multiple pulmonary nodules (< 5 mm diameter) + mosaic attenuation
Mosaicism may be related to endobronchial tumorlets or associated constrictive (obliterative) bronchiolitis
1/3 have asthma
Mastocytosis
Rare disorder with proliferation of mast cells in extracutaneous organs
Lung involvement shows centrilobular nodules and cysts (or emphysema)
Skeletal: Diffuse osteosclerosis from bone marrow infiltration
GI tract and spleen more often involved than lung
Asthma due to excess histamine
Other Essential Information
Acute onset wheezing
Asthma
Congestive heart failure
Pneumonia
Pulmonary embolus
Aspiration syndromes
Foreign body
Insidious onset wheezing
Endobronchial tumor
Congestive heart failure
Extrinsic airway narrowing
Course of symptoms
Intermittent: Asthma, aspiration, pulmonary embolus, congestive heart failure, foreign bodies
Persistent: Asthma, extrinsic or intrinsic airway narrowing, Churg-Strauss vasculitis
Progressive: Asthma, tumors, eosinophilic pneumonia, Churg-Strauss vasculitis
Image Gallery
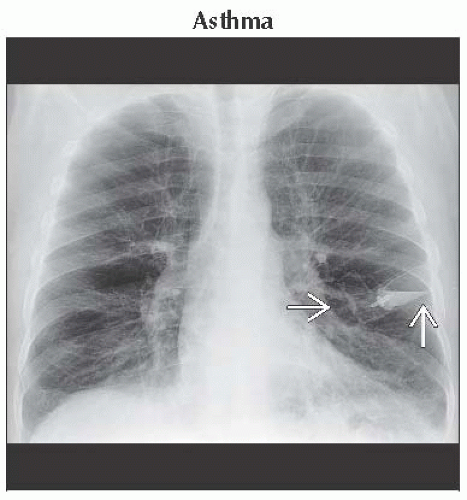 Frontal radiograph shows marked hyperinflation. Note the asthma inhaler  left in shirt pocket. Radiographs have limited utility in asthma, as they may be normal even in patients with status asthmaticus. left in shirt pocket. Radiographs have limited utility in asthma, as they may be normal even in patients with status asthmaticus. |
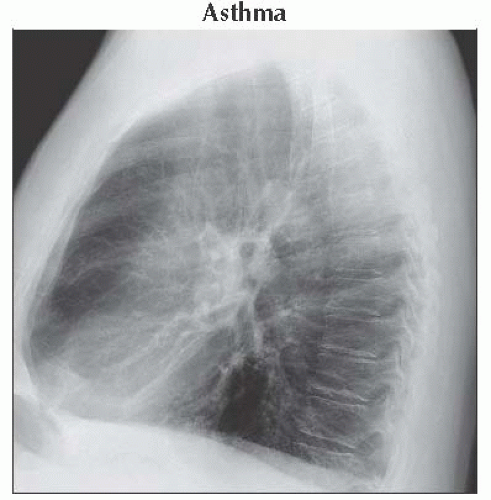 Lateral radiograph shows flattened hemidiaphragms and increased retrosternal lucency. Asthma complications include pneumomediastinum, pneumothorax, atelectasis from mucus plugging, and pneumonia. |
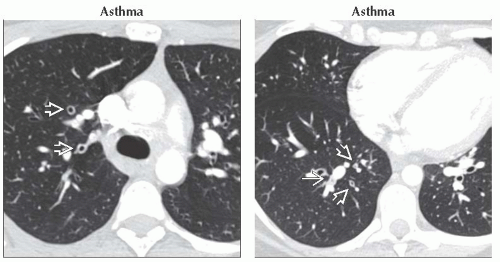 (Left) Axial HRCT shows bronchial wall thickening
 ; other airways are normal. Note that study was CTA for suspected pulmonary embolus. Some airways may be mildly dilated and may reflect bronchodilatation from uninvolved airways. (Right) Axial HRCT shows bronchial wall thickening ; other airways are normal. Note that study was CTA for suspected pulmonary embolus. Some airways may be mildly dilated and may reflect bronchodilatation from uninvolved airways. (Right) Axial HRCT shows bronchial wall thickening  and mucus plugs and mucus plugs  . Mucus plug in this case is not associated with atelectasis. Note that bronchial wall thickening in asthma may be heterogeneous. . Mucus plug in this case is not associated with atelectasis. Note that bronchial wall thickening in asthma may be heterogeneous.Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
 Get Clinical Tree app for offline access
Get Clinical Tree app for offline access

|