Ventricular tachycardia (VT) has many etiologies, but generally occurs in patients with underlying structural heart disease (Table 18.1). This can be acquired or inherited. Myocardial disease and scarring cause abnormal cardiac impulse formation and propagation, which can lead to VT. In developed countries, the most common cause of structural heart disease is coronary artery disease. In patients with coronary artery disease, ventricular fibrillation and polymorphic VT usually are caused by acute ischemia, whereas sustained monomorphic VT usually is caused by reentry around a scar from a previous myocardial infarction.
Other acquired forms of structural heart disease resulting in VT include nonischemic, dilated cardiomyopathy, hypertensive heart disease, valvular heart disease, and certain infiltrative diseases such as sarcoidosis or amyloidosis. Inherited forms of structural heart disease that can cause VT include hypertrophic cardiomyopathy and arrhythmogenic right ventricular dysplasia that is characterized by fatty infiltration and fibrosis.
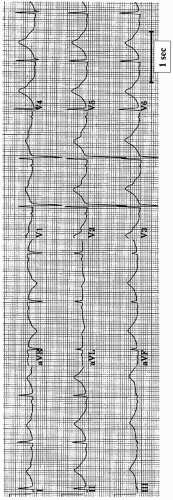
Ventricular tachycardia and fibrillation can also occur in individuals without any apparent structural heart disease. Idiopathic VT most often arises in the outflow tract of the right ventricle or the left posterior fascicle in the left ventricle. A molecular abnormality of one of the cardiac membrane ion channels can also result in VT. More than 170 mutations of genes have been identified as causes of congenital long-QT syndrome (LQTS). Mutations of the potassium channel genes, KvLQT1 and HERG, and the sodium channel gene, SCN5A, account for most cases (Table 18.2). Each LQTS subtype has been associated with a specific T-wave abnormality (1). Polymorphic ventricular tachycardia occurs in these patients as a result of early afterdepolarizations. Brugada syndrome is caused by a sodium channel defect, is manifested as incomplete right bundle-branch block with ST-segment elevation in leads V1 to V3 (Fig. 18.1), and can lead to ventricular fibrillation (2). Catecholaminergic polymorphic VT is characterized by ventricular tachyarrhythmias (predominantly bidirectional VT) that occur during physical activity. This condition is caused by a mutation of the gene encoding for the ryanodine receptor, which is responsible for calcium release from the sarcoplasmic reticulum. The short-QT syndrome is characterized by a QT duration less than 300msec, (3) and is due to a gain-in-function mutation in the KCNH2, KCNQ1, or KCNJ2 gene. All of these genes have been implicated in the long-QT syndrome (Table 18.2), in which loss-offunction mutations are present.
Extrinsic causes of VT include drugs and electrolyte abnormalities. Many cardiac and noncardiac drugs block the potassium channel IKr. Blockade of the potassium current leads to prolongation of repolarization (Fig. 18.2) and can lead to a polymorphic ventricular tachycardia known as torsades de pointes. Commonly prescribed drugs that prolong the QT interval are listed in Table 18.3. A more complete list can be found at www.torsades.org. Factors that predispose to torsades de pointes include female gender, bradycardia, hypokalemia, the administration of more than one QT interval-prolonging drug, and decreased drug clearance. Digitalis toxicity can cause VT by causing delayed afterdepolarizations.
TABLE 18.1.Causes of ventricular tachyarrhythmias
Structural causes
Acquired
Coronary artery disease
Dilated nonischemic cardiomyopathy
Hypertensive heart disease
Valvular heart disease
Infiltrative diseases: sarcoidosis, amyloidosis
Chagas disease
Myocarditis
Inherited
Hypertrophic cardiomyopathy
Arrhythmogenic right ventricular dysplasia
Congenital heart disease
Primary electrical causes
Idiopathic ventricular tachycardia
Idiopathic ventricular fibrillation
Congenital long-QT syndrome
Brugada syndrome
Wolf-Parkinson-White syndrome
Extrinsic causes
Drugs
Hypokalemia
Hypomagnesemia
Hypoxemia
Chest trauma
Asynchronous shock during cardioversion
Central nervous system abnormality
TABLE 18.2.Subtypes of long-QT syndrome
VARIANT
GENE
CHROMOSOME
FUNCTION
LQT1
KCNQ1
11p15.5
IKs alpha subunit
LQT2
KCNH2
7Q35-35
IKr alpha subunit
LQT3
SCN5A
3p21-23
INa alpha subunit
LQT4
ANK2
4q25-2
Targeting protein
LQT5
KCNE1
21p22.1-22-2
IKs beta subunit
LQT6
KCNE2
21p22.1-22-2
IKr beta subunit
LQT7
KCNJ2
17p23.1-24.2
IK1
LQT8
CACNA1C
12p13.3
I Ca alpha subunit
JLN1
KCNQ1
11p15.5
IKs alpha subunit
JLN2
KCNE1
21p22.1-22-2
IKr beta subunit
Adapted from: ACC/AHA/ESC 2006 Guidelines for management of patients with ventricular arrhythmias and the prevention of sudden cardiac death. J Am Coll Cardiol2006;48:5, e247-e346, with permission.
PRESENTING SYMPTOMS AND SIGNS
Patients in whom sustained VT develops can have cardiac arrest, syncope, presyncope, congestive heart failure, chest pain, or palpitations. Sudden death occurs in approximately 400,000 persons in the Unites States annually and is usually caused by ventricular fibrillation. Patients with nonsustained VT are usually asymptomatic but can have palpitations or syncope.
Examination of a patient who is having sustained VT may reveal pulselessness, unconsciousness, pulmonary edema, or signs of shock. When VT is hemodynamically tolerated, signs of tachycardia and atrioventricular dissociation may be present.
HELPFUL TESTS
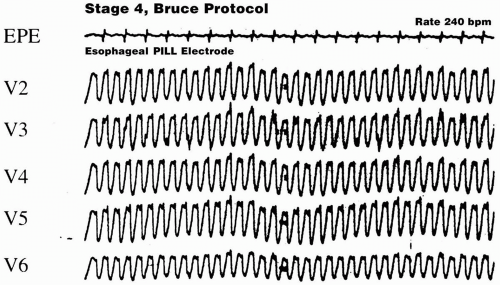
The most useful test in a patient with a sustained VT is an electrocardiogram. A recording of atrial activity during a sustained wide-QRS complex tachycardia with an esophageal electrode (Fig. 18.3) can help establish the presence of atrioventricular dissociation. A recording from a temporary atrial epicardial pacing electrode is valuable in patients who have recently undergone cardiac surgery. Patients with sustained VT or ventricular fibrillation must also undergo a careful physical examination, review of medications, and measurement of electrolytes and cardiac enzymes. Most patients should undergo echocardiography, coronary angiography, and left ventriculography. Holter monitoring may be helpful in identifying VT and quantitating the PVC burden. Patients with frequent idiopathic PVCs (more than 20% of their total QRS complexes) can develop a cardiomyopathy that is reversed by catheter ablation (4). Patients with frequent asymptomatic PVCs should have their left ventricular function assessed periodically to rule out a decline in left ventricular function.
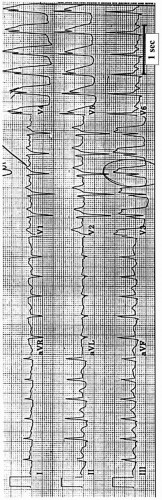
FIGURE 18.1. Twelve-lead electrocardiogram of a patient with Brugada syndrome. Note the incomplete right bundle-branch block with ST-segment elevation and T-wave inversion in leads V1 to V2. Two of the patient’s brothers had died suddenly.
FIGURE 18.2. Electrocardiogram recorded from a patient who was treated with intravenous haloperidol, showing sinus rhythm with marked prolongation of the QT interval.
TABLE 18.3.List of commonly used medications that prolong the QT interval
Cardiac drugs
Procainamide
Quinidine
Disopyramide
Sotalol
Ibutilide
Dofetilide
Amiodarone
Probucol
Noncardiac drugs
Tricyclic antidepressants
Phenothiazines
Haloperidol
Risperidone
Halothane
Terfenadine
Astemizole
Cisapride
Pentamidine
Macrolide antibiotics
Serotonin reuptake inhibitors
FIGURE 18.3. Five-lead electrocardiogram (V2 to V6) of a patient with exercise-induced wide-QRS-complex tachycardia. The top tracing displays recordings from an esophageal pill electrode (EPE) reflecting the left atrial electrograms. A 2:1 ventriculoatrial conduction indicates that this is VT.
The prognosis of a patient with asymptomatic, nonsustained VT depends on the presence or absence of ventricular dysfunction. Therefore, patients with nonsustained VT should undergo testing to evaluate ventricular function and to exclude ischemia. Patients with preserved ventricular function have a good prognosis and usually do not need further testing. Conversely, patients with significant ventricular dysfunction are at increased risk of dying suddenly and should undergo further evaluation. Electrophysiologic testing can be done to risk-stratify patients with coronary artery disease, prior myocardial infarction, and left ventricular dysfunction who experience nonsustained VT. Patients with inducible, sustained VT during programmed electrical stimulation are at high risk for cardiac arrest and benefit from implantation of a prophylactic cardiac defibrillator (5,6,7). Electrophysiologic testing has limited value in the risk stratification of patients with a nonischemic cardiomyopathy.
Noninvasive tests that have been used to risk-stratify patients with nonsustained VT include signal-averaged electrocardiography, measurement of heart-rate variability, and assessment of T-wave alternans. T-wave alternans assesses the fluctuation in the amplitude of T waves during exercise or atrial pacing. This test has been helpful for identifying high-risk patients with ischemic cardiomyopathy (8) and nonischemic cardiomyopathy (9). Risk assessment appears to be independent of ejection fraction, and T-wave alternans testing has a very high negative predictive accuracy.
DIFFERENTIAL DIAGNOSIS
Ventricular tachycardia is defined as three or more consecutive ventricular complexes at a rate greater than 100 beats per minute, and can be categorized on the basis of the morphologic features of the QRS complexes: as monomorphic VT, polymorphic ventricular tachycardia, or ventricular fibrillation. A ventricular arrhythmia is considered sustained when it requires termination, when it results in symptoms, or when it lasts longer than 30 seconds.
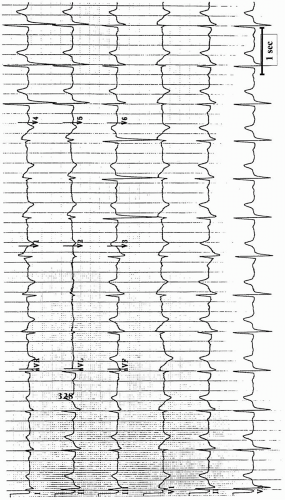
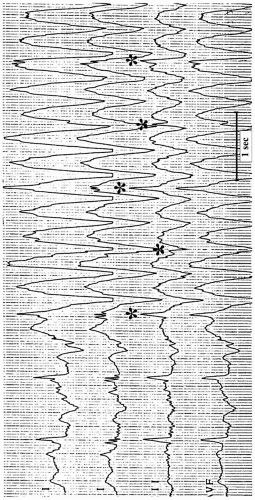
When faced with an apparent wide-QRS complex tachycardia, it is important first to exclude electrocardiographic artifact (10). Artifact can be recognized when portions of the baseline QRS complexes are visible within the suspected wide-QRS complex tachycardia at intervals that are similar to the cycle length of the baseline rhythm (Fig. 18.4). Other clues that suggest artifact include a disturbance of the baseline before the onset, a QRS complex that follows termination of the apparent tachycardia earlier than would be expected, and witnessed body movements during recording. Sinus tachycardia with ST segment elevation can also manifest as a pseudo-wide-QRS complex tachycardia. A 12-lead electrocardiogram identifies ST segment elevation as the cause of the apparent wide QRS complexes (Fig. 18.5).
Monomorphic Ventricular Tachycardia
Monomorphic VT must be distinguished from supraventricular tachycardia with bundle-branch block aberration. Other, less-common causes of a regular, wide-QRS complex tachycardia include antidromic atrioventricular reentrant tachycardia that occurs through an accessory pathway, and ventricular pacing. Antidromic atrioventricular reentrant tachycardia often is indistinguishable from VT.
Differentiation of VT from supraventricular tachycardia with aberrancy is important because of the implications for immediate and long-term treatment. Clinical and electrocardiographic factors must be considered when a wide-QRS complex tachycardia is present. An important principle is that when any uncertainty exists regarding the diagnosis, it is safest to assume that a wide-QRS complex tachycardia is VT. A history of myocardial infarction or congestive heart failure has a positive predictive value of greater than 95% for VT (11). The presence of hemodynamic stability and minimal symptoms should not influence the differentiation of VT from supraventricular tachycardia with aberration (12).
Electrocardiographic findings that support a diagnosis of VT are summarized in Table 18.4 and can be remembered by the alphabetic mnemonic: “ABCDEF.” The principle of each criterion is that when the QRS morphologic pattern does not have features of a typical left or right bundle-branch block pattern, the rhythm is most likely VT. However, many exceptions to these rules are found. Atrioventricular dissociation (“A”) is the most helpful criterion. Unfortunately, atrioventricular dissociation is not present in about one fourth of ventricular tachycardias because 1:1 ventriculoatrial conduction occurs, and it is often difficult to identify unless the tachycardia rate is relatively slow. Signs of atrioventricular dissociation include P waves that are independent of the QRS complexes, capture beats, and fusion beats (Fig. 18.6). The broader (“B”) the QRS complex is, the more likely it is that the rhythm is ventricular tachycardia (Fig. 18.7). A QRS duration exceeding 160 milliseconds for left bundle-branch morphologic patterns and exceeding 140 milliseconds for right bundle-branch morphologic patterns supports a diagnosis of VT. An RS interval (the time from the onset of the R wave to the nadir of the S wave) in the precordial leads that exceeds 100 milliseconds is consistent with VT (13). Concordance (“C”) is defined as the presence of QRS complexes that are all upright or all inverted in the precordial leads and is a sign of VT. Bundle-branch block patterns do not demonstrate concordance because they usually have at least one biphasic complex in the precordial leads. Deviation (“D”) of the axis in a direction that is not typical for a bundle-branch block pattern, such as right-axis deviation with a left bundle-branch block pattern, suggests ventricular tachycardia.
FIGURE 18.4. Four-lead rhythm-strip of electrocardiographic artifact simulating monomorphic ventricular tachycardia. A diagnosis of artifact can be made on the basis of identification of portions of QRS complexes (asterisks) at intervals that correspond to the baseline sinus-cycle length. Note the unstable baseline before the onset of the apparent tachycardia.
FIGURE 18.5. Twelve-lead electrocardiogram recorded in a patient with an acute anterior myocardial infarction. A single, modified chest-lead recording from the same patient appeared to demonstrate a wide-QRS complex tachycardia that was actually sinus tachycardia with prominent ST-segment elevation.
TABLE 18.4.Electrocardiographic findings that support a diagnosis of ventricular tachycardia
Atrioventricular dissociation
Broad
Concordance
Deviation of axis
Effect of maneuvers
Features of the QRS complex
Only gold members can continue reading. Log In or Register to continue