Chapter 61 Vascular Trauma
Treatment of vascular trauma in the civilian and military venues has had a symbiotic relationship. Although German surgeons accomplished a limited number of arterial repairs in the early part of World War I, ligation of major arterial injuries was not abandoned until the Korean Conflict in the 1950s. Until that time, arterial ligation was used preferentially, and some experts of the day felt there was little place for definitive arterial repair of the combat wound. Review of the arterial injuries during World War II revealed that arterial ligation was followed by gangrene and amputation in half the cases.1 After World War II, significant advances made in civilian hospitals included atraumatic vascular clamps, monofilament sutures, arteriography, and prosthetic grafting. These advances made it possible to repair arterial injuries in the battlefield, such that during the Korean conflict, the overall amputation rate was reduced to 13%.2 The latest innovation in vascular surgery, the “endovascular revolution,” is rapidly changing our approach to managing some components of vascular trauma in the civilian setting.3 It is unclear to what extent these techniques will facilitate care in the battlefield.
Trauma remains the leading cause of death in the 15- to 44-year-old age group in the United States. The prevalence of iatrogenic vascular injury has increased in tandem with the number of catheter-based invasive procedures.4 Overall, arteries in the lower extremities are injured more than other anatomical areas. In this chapter, the basic definitions and treatment strategies for vascular trauma are described.
Basic Concepts and Definitions
Signs of Vascular Trauma
The hard signs of vascular trauma warrant urgent or immediate operative exploration and intervention (Box 61-1). In many instances, these patients present with systemic shock, and resuscitative efforts are best coordinated in the operating room. The soft signs of vascular injury (see Box 61-1) require further diagnostic evaluation to plan intervention if needed. Depending on the hemodynamic status of patients with soft signs of vascular injury, subsequent evaluation may include invasive or noninvasive imaging techniques.
 Box 61-1
Box 61-1Hemorrhagic Shock
Hemorrhagic shock is a condition of reduced tissue perfusion due to inadequate delivery of oxygenated blood, resulting in anaerobic metabolism, acidosis, and deleterious alterations to cell function. Because bleeding may be a major complication associated with vascular trauma, it is important to provide information on the kinds of shock that may be associated with these injuries. There are four types of hemorrhagic shock, ranging in severity based on the amount of blood lost. Clinical characteristics associated with the degree of hemorrhagic shock are described in Table 61-1.
Ischemia/Reperfusion Injury
Ischemia/reperfusion is a complex pathological process involving intracellular and extracellular processes that result in metabolic, thrombotic, and inflammatory changes in brain, intestine, heart, kidney, and skeletal muscle. A devastating component of ischemia/reperfusion injury is the paradoxical increase in tissue injury associated with restitution of blood flow to ischemic tissues. The myonephropathic-metabolic syndrome was described by Haimovici in a few patients who underwent lower-extremity revascularization following acute ischemia in the late 1950s, providing one of the first published clinical observations of limb ischemia and reperfusion.5,6 These patients experienced ongoing lower-extremity necrosis and myoglobin-induced renal failure in the presence of palpable pulses.
One of the most severe components of ischemia/reperfusion injury, the paradoxical decrease in blood flow following restoration of perfusion, was described initially as a no-reflow phenomenon in the brain,7 and May et al. described the same phenomenon 10 years later in skin flaps.8 These investigators described cellular swelling, intravascular aggregation of cellular components of blood (platelets, neutrophils), and leakage of intravascular fluid into the interstitial space as basic mechanisms whereby tissue flow is decreased during reperfusion, providing the first definitive histological evidence to support the existence of the no-reflow phenomenon. From a biochemical perspective, it is useful to discuss this process in terms of its components: ischemic injury and reperfusion injury.
Compartment Syndrome
Acute compartment syndrome is a surgical emergency. Compartment syndrome may be defined as increased tissue pressure in a closed myofascial space, resulting in disturbed microcirculation that leads to irreversible neuromuscular ischemic damage.9 Acute compartment syndrome most commonly occurs following lower-limb trauma. Emergency decompression through open and extensive fasciotomies is the treatment of choice. The cardinal clinical feature is severe pain, greater than would be expected from the original insult. The pain may be exacerbated by passive extension of the tendons crossing the symptomatic compartment or arising from the muscles within it. Among other clinical features, the first is usually hypoesthesia, followed by compartment distension and muscle weakness in the later stages. The need for prompt intervention and the benefits of timely surgical decompression require a high index of suspicion and effective clinical assessment to make the diagnosis. Clinical assessment may be supported by compartment pressure measurements, in which a needle is inserted into the compartment and pressure monitored using a pressure transducer. The pressure that indicates a need for fasciotomy has not been universally established, although a pressure greater than 30 mmHg is widely accepted as abnormal. Other authors advocate a threshold that relates to the diastolic blood pressure, with compartment pressures within 30 mmHg of the diastolic pressure indicating a need for fasciotomy.
A recent 10-year review of the incidence of compartment syndrome in a mature level I trauma center indicated that after lower-extremity trauma, 2.8% of patients will require fasciotomy. A stepwise logistic regression identified the presence of vascular injury (arterial, venous, or combined), need for packed red blood cell (RBC) transfusion, male gender, open fracture, elbow or knee dislocation, and age younger than 55 as independent predictors for the need for fasciotomy after extremity trauma. Combined arterial and venous injury resulted in fasciotomy in 42% of patients.10
Thoracic Vascular Injury
With the heart, great vessels, brachiocephalic vessels, and descending aorta housed within the confines of the thorax, mortality following vascular injury is associated with exsanguinating hemorrhage at the scene. Hemothorax associated with penetrating trauma can be managed with a chest tube, but if a major vascular structure is involved, patient survival is largely dependent on whether there is free hemorrhage or a contained hematoma. It is estimated that over 80% of patients suffering blunt trauma to the aorta will die at the scene of the accident.11
Thoracic/Cardiac Box
Thoracic aorta
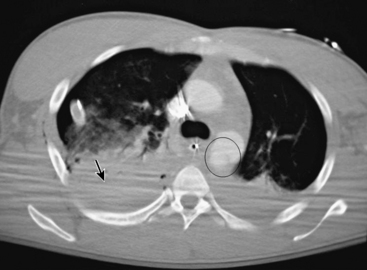
Traumatic aortic rupture is a devastating clinical problem that is difficult to manage owing to the need to approach aortic repair in concert with management of complex associated injuries to nonvascular organ systems (Fig. 61-1). The natural history of aortic transection is relatively self-selective, with a significant majority of patients exsanguinating at the scene. Of those who make it to the hospital alive, upwards of 38% die largely as a result of associated injuries.12 Fabian et al. estimate the incidence of traumatic aortic disruptions in the United States to be between 7500 and 8000 patients annually; about 1000 to 1500 of these patients arrive at hospitals alive.13 It took 50 centers 2.5 years to generate 274 patients for this prospective report. This averages just over two patients per year per center. Despite the low volume, contemporary analysis reveals that of the 9% to 19% who reach the hospital alive,14 approximately 30% will die within the next 6 hours, and a total of 50% within 24 hours.15
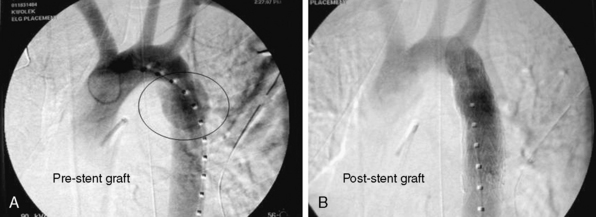
Until recently, open operative intervention for these traumatic injuries required thoracotomy, anticoagulation, and application of an aortic cross-clamp. These operative maneuvers conceded the potential of exacerbating associated injuries and spinal cord injury.13,16,17 Proximal-to-distal aortic bypass using a Gott Shunt, left heart bypass with heparin-bonded circuits, and cardiopulmonary bypass (CPB) may all significantly reduce the likelihood of paraplegia.18,19 Thus, the current status of traumatic aortic disruption and traditional repair is not ideal. Advances in endovascular repair techniques for traumatic rupture have resulted in a major change in the approach to treatment of this devastating clinical entity.20–22 This change in approach is based on and supported by improved mortality associated with repair by endovascular vs. open techniques in patients with multiple trauma23 (Fig. 61-2).
Open Surgical Approach
Open repair may be accomplished either with direct cross-clamping alone or with circulatory assistance (left-sided heart bypass with heparin-coated conduits, cardiopulmonary bypass, or femoral-femoral bypass).19,24,25 Optimal exposure of the thoracic aorta is gained through a posterolateral thoracotomy with an incision in the fourth intercostal space. The aortic arch may be controlled either with clamping between the left common carotid and left subclavian, or just distal to the left subclavian artery. The descending thoracic aorta is controlled distally immediately after the traumatic injury to avert sacrifice of the intercostal arteries. The aorta can then be repaired with direct suturing or graft interposition.
Endovascular Approach
Trauma centers equipped with radiographic fixed or mobile C-arms and angiographic equipment in the operating rooms would be ideal. This affords the opportunity for patients to be treated for their vascular injury(s) via open cutdown or percutaneously in a setting where surgical interventions for associated injuries may also be treated if indicated at that time.26 Though not specifically designed to treat thoracic aortic transections, the use of endoluminal abdominal aortic extension cuffs has been shown to be technically feasible in several small series.26–28 This has been particularly evident in young individuals with normal-sized aortas. Broad prepping and draping of the patient should be undertaken so that emergent intervention for associated abdominal or thoracic injuries can be pursued while the patient is under anesthesia. Patients should be placed supine on the appropriate x-ray table, with slight rotation to a decubitus position. This orientation of the patient provides access to the femoral and iliac vessels and the abdominal aorta if needed.
The diameter of stent grafts should be oversized at least 20% based on sizing obtained from computed tomographic angiography (CTA). Unlike treatment of patients with degenerative aneurysms, the aortic diameter proximal to the injured aorta is most often in the 18- to 26-mm range. Generous oversizing can lead to collapse of a stent graft.29
Thoracic venae cavae
Simple isolated injuries to the thoracic venae cavae can be managed with lateral venorrhaphy. Partial-occluding clamps or temporary inflow occlusion can be used in these circumstances to facilitate repair.30 Complex injuries to the venae cavae or associated injuries to the heart may require CPB and/or interposition grafts for exposure and repair.
Pulmonary vessels
Trauma to the main right or left pulmonary arteries is extremely rare and almost exclusively found after penetrating traumatic injury. Some case reports have described blunt traumatic injury to the main pulmonary arteries, but it remains exceedingly rare.31 As with many of the great vessel injuries, cardiac tamponade or hemopericardium is the common presenting finding. Usually the diagnosis is made in the operating room during an empirical thoracotomy for hemopericardium. Distal pulmonary vascular injuries beyond the mediastinum can be seen following both blunt and penetrating trauma. Extensive vascular injury or significant injury to the hilar region may necessitate a pneumonectomy, which bears a significantly high mortality rate in trauma situations.32
Carotid and Vertebral Vascular Trauma
Penetrating Carotid Artery Trauma
Stab and low-velocity missile wounds account for the vast majority of civilian penetrating carotid artery injuries. Demographics of the injured generally include young, healthy males and associated alcohol and/or illegal drug use precipitating the injury. Studies have shown that carotid injuries occur in roughly 17% of all penetrating neck trauma.33 Common carotid artery (CCA) injury is more frequent than internal carotid injuries. Iatrogenic injury to the carotid artery is most commonly due to attempted central venous catheter insertion.
Anatomical considerations
The neck is divided anatomically into three zones of injury (Box 61-2). Zone I comprises the area from the thoracic outlet (the level of jugular notch) to the cricoid cartilage, zone II begins at level of the cricoid cartilage and terminates at the angle of the mandible, and zone III extends from the angle of the mandible to the skull base. The zone divisions were based on the anatomical relationships of the neurovascular and aerodigestive tract structures, as well as the surgical approach for exposure.
 Box 61-2
Box 61-2Zone II Injuries
In stable patients, the management of zone II injuries of the neck is the source of some debate among trauma centers. Historically, all zone II injuries were operatively explored because of improved mortality rates with immediate operative intervention, as opposed to delayed or expectant intervention.34 The relative ease of operative exposure in zone II and low morbidity rate with operation, coupled with the many vital structures passing through this region, made it the mainstay of treatment for many years, despite the high negative exploration rate. With advancements in diagnostic imaging, selective exploration has become more popular in stable patients. Thus, the decision whether operative exploration is necessary can be predicated on further diagnostic evaluation and imaging to confirm or rule out vascular injury. Usually this evaluation includes serial physical examinations, esophagoscopy, bronchoscopy, and imaging studies (i.e., catheter-based angiography, CTA, magnetic resonance angiography [MRA], or duplex ultrasound scanning) when vascular injury is suspected.33,35–37 Centers that have used angiography to evaluate penetrating neck injuries in hemodynamically stable patients have found that only 13% to 17% of these patients have major vascular (carotid and vertebral) injuries requiring repair.33,37 Because of this, some have begun to advocate angiography only in cases of suspected vascular injury and report very few missed injuries with this approach. More recent studies have also advocated CT scanning as an adjunct to the physical examination in zone II neck injuries, but angiography remains the gold standard.
Operative approach/open surgical management
The surgical approaches for zone I and III injuries can be significantly more complicated and challenging. To obtain adequate proximal vascular control and exposure, vascular injuries within zone I frequently require a median sternotomy or supraclavicular “trap-door” incision in addition to the standard cervical oblique incision. Zone III injuries may necessitate cephalad extension of the exposure to attain distal vascular control. Maneuvers such as dislocation or partial resection of the mandible are not infrequent, especially in high zone III injuries. Temporary control of bleeding at or near the skull base can be accomplished through insertion and inflation of a Fogarty catheter into the injured vessel.38
Endovascular management
Though endovascular management is less prevalent in blunt carotid injury, it has provided some promising results in the management of penetrating carotid trauma, especially in zone I and high zone III (internal carotid artery [ICA]) injuries.39,40 Traditionally, ICA injuries (pseudoaneurysm and dissections), albeit rare, warrant anatomical reconstruction to prevent devastating ischemic neurological insults. Operating high in the neck is technically demanding and can be associated with cranial nerve injury; thus, endovascular stenting and coiling has the potential to limit iatrogenic damage associated with open exploration. Recent reviews have demonstrated that stent graft placement for traumatic ICA pseudoaneurysms have been successful in neurologically symptomatic patients following trauma.41,42 Consideration must be given to thromboembolic events associated with stent graft placement, the potential for intimal hyperplasia formation, and restenosis. The anatomical tortuosity of the vessel may prevent safe crossing of the traumatic lesion with a guidewire. A recent retrospective review of 113 patients with blunt or penetrating carotid injury demonstrated a promising short-term patency (up to 2 years) of carotid stent grafts (80%).43
Blunt Carotid/Vertebral Artery Injury
Blunt carotid and vertebral artery injury (BCVI) is diagnosed roughly once in every 1000 patients.44 Though BCVI is considered a rare occurrence, without prompt and appropriate care, cerebral ischemia rates range from 40% to 80%, and mortality rates from 25% to 60%.44,45 BCVI lesions vary in mechanism and location; skull base fractures, for example, can contuse the intrapetrous/cavernous portion of the internal carotid artery. Blunt trauma to the carotid artery can be induced via a stretching, twisting, or shearing effect to the neck. BCVI after strangulation and choking has been described as well.45 Several authors have proposed signs, symptoms, or injury patterns that should raise the suspicion for BCVI.44,46,47 Skull base, midface, mandible, and cervical spine fractures are associated with BCVI and should raise a healthy concern. Significant blunt trauma to the chest and neck in a patient with a Glasgow Coma Scale score of 8 or less represents another clinical scenario that warrants further investigation. Note that these injuries can also be insidious in their presentation, so in a patient with a Glasgow Coma Scale score above 8 but a history of a high-risk mechanism (motor vehicle accident/deceleration injury) and/or trauma to the face and neck, suspicion for BCVI should remain.
Diagnostic evaluation
In most emergency situations, multidetector CTA remains the initial tool for evaluation of carotid injuries because it can often be performed expeditiously near or in the emergency room. Adequacy of the older single-slice helical CTA in diagnosing BCVI was limited by sensitivities and specificities of 68% and 67%, respectively.48 However, several studies have shown the effectiveness of 16-channel multislice CTA in diagnosis of BCVI,44,49 with sensitivities and specificities each greater than 94%. The somewhat subtle nature of blunt carotid injury makes digital subtraction angiography (DSA) the gold standard for the diagnosis of blunt carotid injury. Imaging by CTA may be compromised in situations where metallic artifact is present (shrapnel, plates, prosthesis, etc.). Although DSA is an invasive method, it not only depicts the extent and severity of vessel injury, it can also provide information about the integrity of cerebral circulation. Magnetic resonance angiography is another safe, noninvasive technique that can provide data concerning vessel morphology and blood flow. Its accuracy in diagnosing BCVI may rival that of CTA, but time required for the examination, difficulty monitoring the patient during the study, and high cost limit its use.45 Duplex ultrasonography is used more in penetrating carotid trauma but is not sensitive enough to be the screening modality of choice in BCVI.44
Classification of blunt carotid injury: the Denver scale
The Denver Scale (Table 61-2) has been widely accepted and used to classify blunt carotid injury.50 It was employed to standardize and direct care for the different grades of vessel injury based on multiplanar CTA or DSA findings. Grade I to IV injuries typically warrant anticoagulation as the mainstay of treatment, with consideration of surgical intervention if contraindication of anticoagulation or further neurological deterioration exists. Grade V injury, which represents complete transection with extravasation, is most appropriately treated through surgical intervention, whether it be an endovascular or open approach.
Table 61-2 Denver Scale for Blunt Carotid Injury
| Type/Grade | Radiological/Angiographic Findings and Criteria |
|---|---|
| I | Vessel wall irregularity or dissection/intramural hematoma with <25% luminal stenosis |
| II | Presence of intraluminal thrombus, raised intimal flap, or dissection/intramural hematoma with ≥25% luminal stenosis |
| III | Presence of pseudoaneurysm |
| IV | Vessel occlusion |
| V | Complete transection with extravasation |
From Biffl WL, Moore EE, Offner PJ, et al: Blunt carotid arterial injuries: Implications of a new grading scale. J Trauma 47:845–853, 1999.
Clinical management
Despite increased awareness of blunt carotid injury, there is no agreement on the best therapeutic approach. Accumulated data suggest that conservative therapy using antithrombotic therapy with heparin prevents cerebral infarction. Similarly, antiplatelet therapy and anticoagulation with warfarin (international normalized ratio [INR] 2-3) were equally effective in reducing risk of stroke following BCVI.45,51 In a recent analysis of the national trauma database, a comparison of functional independence following BCVI in patients treated conservatively (anticoagulation and/or antiplatelet agents) vs. operatively (open and endovascular treatment) was performed.52 There was no difference in functional outcome in these patients, regardless of conservative or operative intervention. The only demographic difference among the groups was greater injury severity score in patients undergoing endovascular repair. In most studies, BCVI in surgically accessible areas are treated operatively; however, the vast majority of BCVI lesions occur in surgically challenging areas high within the carotid canal or foramen transversarium. Such locations make standard operative approaches for thrombectomy or reconstruction difficult.53
Abdominal Vascular Injuries
Abdominal vascular injury represents 5% to 25% of all abdominal traumatic injuries54 and carries a mortality rate of 31% to 87%.55 With penetrating trauma overwhelmingly the most common etiology of traumatic vascular injury (>90% of cases), any penetrating injury to the torso from the upper thigh to the level of the nipples should generate high suspicion for vascular injury.56 Most patients with major abdominal vascular injury present with a contained or partially contained retroperitoneal hematoma. Patients who suffer major free intraperitoneal hemorrhage frequently die at the scene of injury. Patients with free retroperitoneal or intraabdominal hemorrhage who make it to the hospital usually present with profound hypotension in class IV hemorrhagic shock.56 The incidence of arterial and venous injury is similar and depends on the location, force, and mechanism of the insult. The association of abdominal vascular trauma with assault and aggressive behavior accounts for a shocking 90% to 95% of cases.55
When vascular injury is present in the abdomen, the aorta and IVC are most commonly injured—25% and 33%, respectively.57 The overall mortality rate from penetrating abdominal vascular injuries is 45%, but associated injuries to the abdominal aorta, hepatic veins, retrohepatic vena cava, and/or the portal vein can elevate it to as high as 90%.35,54 Despite our advances in technology and surgical/medical techniques, no significant changes have occurred with regard to mortality associated with abdominal vascular trauma over the last 20 to 30 years. This reflects the lethal potential of these injuries and the fact that patients presenting in shock with vascular injury continue to have a high mortality rate.58
Clinical Presentation and Evaluation
Of those patients with abdominal vascular injury who make it to the hospital, about 14% will lose vital signs en route; thus, minimizing the time from injury to delivery at a medical care facility can result in a significant improvement in outcomes.59 In addition to prehospital time, the clinical presentation will depend on the mechanism of injury, vessel injured, severity of the injury, and presence of other associated injuries. Blunt trauma causes vascular injury through rapid deceleration, anterior/posterior crushing, or laceration from sharp bony fractures. These patients often initially present with stable vital signs, but may rapidly decompensate because of the insidious evolution of blunt abdominal trauma. In contrast, penetrating vascular trauma to the abdomen presents in a less subtle manner.
Regardless of the mechanism, operative exploration is paramount and must be done expeditiously, foregoing any diagnostic imaging in a hemodynamically unstable patient with suspected abdominal vascular injury. Cautious resuscitation is prudent in hemodynamically unstable patients. Excessive fluid resuscitation of an actively hemorrhaging patient can potentiate ongoing blood loss and coagulopathy.60–62 To maintain end-organ perfusion until definitive control of hemorrhaging is obtained, cessation of bleeding and permissive hypotension should be the initial goals of resuscitation.
Retroperitoneal hematomas
Retroperitoneal hematomas occur in more than 90% of abdominal vascular injuries.59 The retroperitoneum is divided into three main zones of injury: zone I is the central/midline retroperitoneum, zone II encompasses the perinephric space, and zone III comprises the pelvic retroperitoneum. Treatment of retroperitoneal hematomas varies depending on the anatomical location and mechanism of injury.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


