Vascular Access Evaluation
ANNA SATTAH and WORTHINGTON SCHENK III
Presentation
A 71-year-old right-handed male is referred for evaluation for arteriovenous (AV) fistula creation for dialysis access. He had a right-sided Cimino radiocephalic wrist fistula created at an outside hospital 3 months ago, which has failed to mature. He is not currently on dialysis; however, his estimated GFR is 16 mL/min/1.7 m2, down from 20 prior to his last operation. His past medical history is significant for hypertension, insulin-dependent diabetes, peripheral vascular disease, and recurrent foot infections resulting in a left below-knee amputation (BKA). He denies any history of central lines in the neck but does report having had a right-sided peripheral inserted central catheter (PICC) line for intravenous (IV) antibiotics. On physical examination, the incision over his Cimino fistula is well healed, but there is no thrill. He has a scar on his right upper arm, which he confirms is from his prior PICC line. He has no other visible scars on his arms or neck. His BKA site is well healed. His pulse exam reveals normal radial and brachial pulses bilaterally. Allen’s test is normal bilaterally.
Imaging
A duplex ultrasound including vein mapping of both arms is obtained. On the right, a thrombosed radiocephalic fistula is seen in the forearm. Flow remains intact in the radial artery distal to the fistula. At the antecubital fossa, the brachial artery internal diameter measures 3.2 mm without evidence of calcifications, and the median antecubital vein measures 3.6 mm. In the upper arm, the cephalic vein measures 2.8 mm. The basilic vein measures 3.4 to 3.9 mm with a focal stenotic lesion narrowing to 2.2 mm corresponding to the site of his prior PICC line. On the left, see Figure 1: in the forearm, the radial artery measures 1.8 mm, and the cephalic vein measures 1.6 mm. At the antecubital fossa, the brachial artery measures 4.2 mm without calcifications, and the median cubital vein measures 4.0 mm. In the upper arm, the cephalic vein measures 2.8 mm. The basilic vein measures 4.6 to 5.5 mm without focal stenoses and remains separate from the deep brachial system into the axilla.
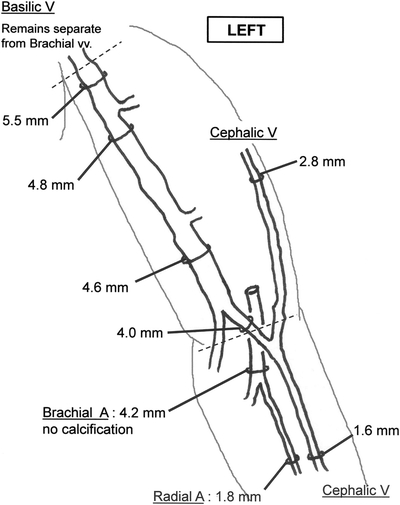
FIGURE 1 Preoperative sonographic evaluation. A Cimino fistula in the left forearm appears a poor choice due to small size of both artery and vein. An upper arm brachiocephalic fistula is possible but runs a substantial risk of nonmaturation due to the small size of the cephalic vein. The anatomy looks favorable for a one-stage basilic vein transposition: the vein diameter is favorable, the antecubital branch (4.0 mm) can be included to gain additional length, and the basilic vein remains separate from the brachial veins.
It is useful to perform an ultrasound evaluation at the initial office visit, which allows for the opportunity to depict the size, course, and location of branches of the veins as well as the size, course, and character of the flow signal of the arteries (Fig. 1). Venous branches near the proposed anastomosis are important to identify for two reasons. First, they can be used to form a Carrel patch when creating an anastomosis. Second, large intact branches may form alternate venous drainage sites and lead to nonmaturation of the fistula.
Recommendations
While there are no well-established evidence-based ultrasound criteria for successful fistula construction, adequate flow through the fistula must be established in order to dilate the venous channel. Suggested sonographic exclusion criteria for creation of autologous fistulas are listed in Table 1. When patients do not fit criteria for a fistula, a PTFE graft should be considered in order to avoid permanent percutaneous catheters.
TABLE 1. Sonographic Exclusion Criteria for Fistula Construction a
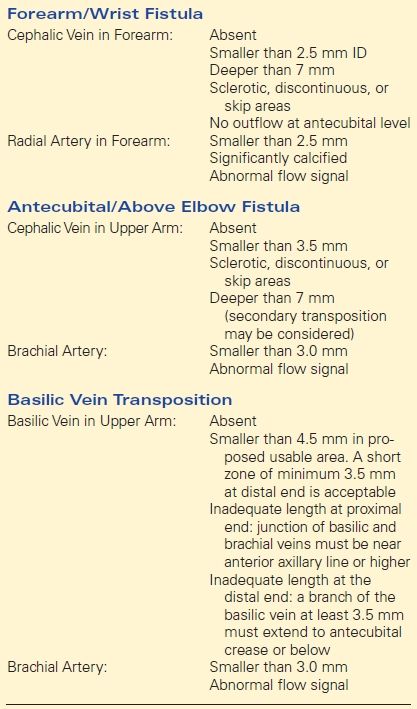
a This table represents an example of sonographic exclusion criteria, intended as an illustration only, not as a recommendation. The criteria are guidelines only and not based on evidence-based data.
Based on his preoperative ultrasound, there are no appropriate autologous options in the right upper extremity. In the forearm, the Cimino fistula has failed. In the upper arm, the cephalic vein is only 2.8 mm, and the basilic vein is small and has a stenotic lesion from a prior PICC line.
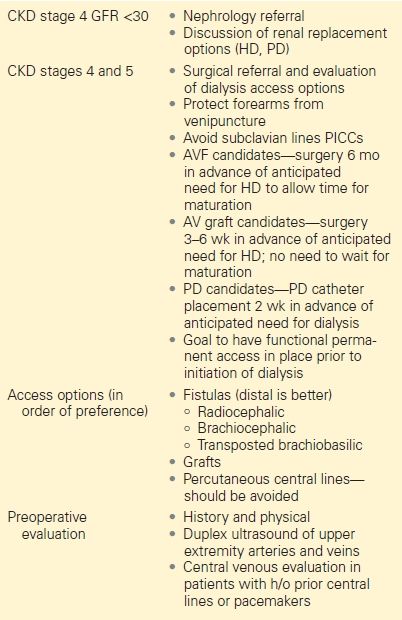
On the left, in the forearm, the radial artery is only 1.8 mm, and in the upper arm, the cephalic vein is only 2.8 mm. The basilic vein, however, looks good (greater than 4.5 mm). These ultrasound evaluations can be done by the surgeon or by a trusted vascular lab and are recommended for preoperative planning. This patient is not yet on dialysis but has progressive stage IV chronic kidney disease (CKD). Based on the National Kidney Foundations 2006 Kidney Disease Outcomes Quality Initiative (KDOQI) guidelines (Table 2), he is appropriate for surgical evaluation and angioaccess construction. He has a reasonable conduit for creation of a basilic vein transposition, and he is scheduled for surgery.
TABLE 2. National Kidney Foundation 2006 KDOQI Guidelines for the Creation of AV Fistulas in Patients with Chronic Kidney Disease