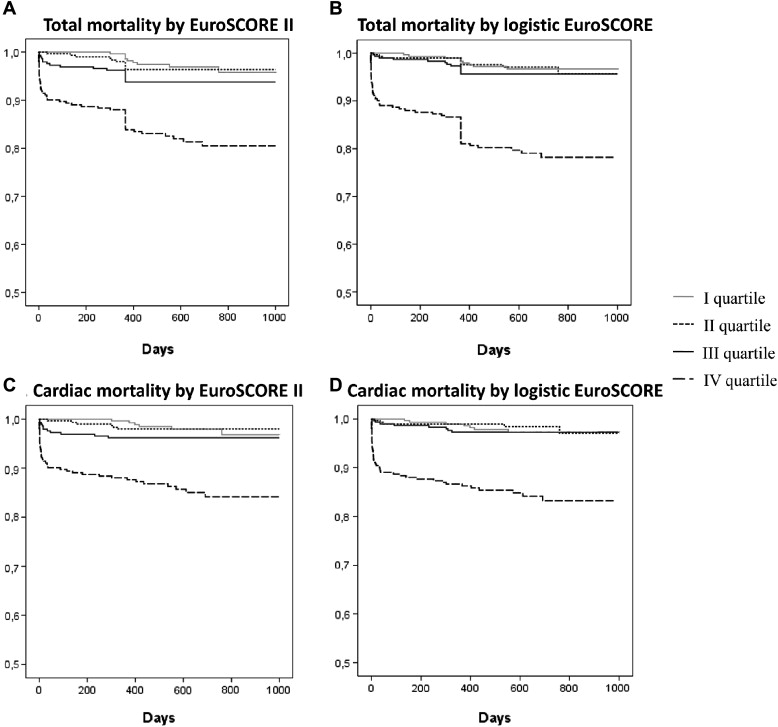
We read the report by Capodanno et al exploring the role of the European System for Cardiac Operative Risk Evaluation (EuroSCORE) II in a series of 537 patients undergoing percutaneous coronary interventions (PCIs). In this study, the recently launched EuroSCORE II was found to significantly correlate with all-cause mortality at 30 days, 1 year, and 5 years. Interestingly, EuroSCORE II showed a better calibration than the logistic EuroSCORE at 30 days, but not at longer follow-up times. The evaluation of the usefulness of EuroSCORE II in surgical populations is underway and its superiority over EuroSCORE (standard or logistic) in predicting mortality is still debated. In this context, with the aim of further assessing its role in PCI setting, we investigated the ability of EuroSCORE II to predict total and cardiac long-term mortality in a study population of 1,170 consecutive patients with coronary artery disease undergoing PCI. The logistic EuroSCORE was prospectively assessed in consecutive patients undergoing PCI from April 2005 to October 2006 at our institution. The characteristics of this study population and the correlation between risk scoring and in-hospital and long-term clinical outcomes have been previously reported. We used clinical records to retrospectively calculate the novel EuroSCORE II of each patient enrolled in this study. Cardiac and total mortality occurring during follow-up (633 ± 168 days) were selected as study end points. A total of 91 patients (0.08%) died during the follow-up and 56 patients (0.05%) had established cardiac cause of death. As the first observation, in the same study population, mean EuroSCORE II was 2.535 ± 4.215, whereas mean logistic EuroSCORE was 6.339 ± 9.777, thus showing a strikingly lower predicted average mortality. This finding extends to the PCI setting a reduction in risk overestimation for the novel risk scoring system. To assess the ability to predict mortality across different levels of baseline risk, the study population was divided into quartiles of risk according to both logistic EuroSCORE (group I, 0 to 1.614; group II, 1.614 to 3.048; group III, 3.048 to 6.35; and group IV, >6.351) and EuroSCORE II (group I, 0 to 0.93; group II, 0.93 to 1.322; group III, 1.322 to 2.425; and group IV, >2.425). Kaplan-Meier survival curves free from death and from cardiac death are reported in Figure 1 and show that most of the discriminatory potential of EuroSCORE II is confined to patients belonging to the higher risk quartile (similar to the old logistic EuroSCORE). In keeping with this, the area under the receiver operating characteristic curve for EuroSCORE II and logistic EuroSCORE for the prediction of cardiac death (0.773, 95% confidence interval [CI] 0.703 to 0.842 and 0.774, 95% CI 0.702 to 0.847, respectively) and total mortality (0.744, 95% CI 0.685 to 0.802 and 0.756, 95% CI 0.696 to 0.816, respectively) were similar (p = 0.94 for cardiac mortality and p = 0.43 for total mortality).