Circulating total free fatty acid (FFA) levels are elevated early in myocardial infarction (MI) and have been associated with an increase in mortality. We investigated the association of serum unbound FFA (FFA u ) levels with mortality in patients presenting with ST-segment elevation MI in the Thrombolysis In Myocardial Infarction II trial. The Thrombolysis In Myocardial Infarction II trial enrolled patients within 4 hours of chest pain onset. The patients were treated with a recombinant tissue plasminogen activator within 1 hour of enrollment. The FFA u concentration was evaluated in serum samples from 1,834 patients obtained at baseline, before therapy. The FFA u level was an independent risk factor for death as early as at 1 day of hospitalization and continued to be an independent risk factor for the >3.8 years of follow-up. When adjusted for other cardiovascular risk factors, the FFA u levels in the fourth versus the first quartile remained an independent risk factor for death from MI (hazard ratio 5.0, 95% confidence interval 1.9 to 13.0), all cardiac death (hazard ratio 2.4, 95% confidence interval 1.3 to 4.4), and all-cause death (hazard ratio 1.9, 95% confidence interval 1.2 to 3.1). Women were twice as likely to be in the upper 2 FFA u quartiles and had approximately twice the rate of death as men. In conclusion, FFA u elevation is 1 of the earliest molecular biomarkers of mortality in patients with ST-segment elevation MI and was independent of other risk factors known to affect the outcomes after ST-segment elevation MI.
Plasma free fatty acid (FFA) levels are elevated early after acute myocardial infarction (MI) and have correlated with increased rates of arrhythmias and mortality, particularly within the first 12 hours. The MI-associated FFA increase occurs primarily through catecholamine activation of adipose tissue lipolysis rather than FFA release from the ischemic cardiac tissue. Although most plasma FFA is bound to albumin, a small fraction (<10 −4 ) is unbound FFA (FFA u ). FFA u levels increase exponentially with an increasing ratio of total FFA to albumin; thus, FFA u is more sensitive to physiologic changes than total FFA. FFA u levels increase rapidly, within 30 minutes of cardiac ischemia induced by balloon angioplasty. We investigated whether the FFA u levels from patients in the Thrombolysis In Myocardial Infarction (TIMI) phase II trial of ST-segment elevation MI (STEMI) could provide an independent assessment of risk of poor outcomes as early as 24 hours after symptom onset.
Methods
The TIMI II trial treated 3,262 patients who had presented within 4 hours of STEMI onset with an intravenous recombinant tissue plasminogen activator plus heparin. After recombinant tissue plasminogen activator therapy, the patients were randomly assigned to either percutaneous coronary intervention or a conservative strategy in which only patients exhibiting ischemia (13%) underwent percutaneous coronary intervention. The TIMI investigators recorded the demographics, medical history, and outcomes for a follow-up period of 3.8 years. A limited access data set of the patient parameters was available for the present study.
Measurements were performed on serum samples (baseline) drawn before recombinant tissue plasminogen activator and heparin therapy. The serum was collected from the patients with STEMI by the TIMI investigators and maintained at −70°C by the National Heart, Lung and Blood Institute (National Institutes of Health, Bethesda, Maryland) blood specimen repository. A subset of these specimens from 2,500 patients was provided by the National Heart, Lung and Blood Institute. The link between patient information and blood specimen tube identification was maintained separately by the Maryland Medical Research Institute (Baltimore, Maryland). After our results had been deposited with the National Heart, Lung and Blood Institute, the linkage was unblinded. Complete patient information from the limited access data set was available for 1,834 patients of the 2,500 baseline blood specimens. Thus, we have reported the results for these 1,834 patients. The present study complied with the Declaration of Helsinki, and the institutional review board committee of the Torrey Pines Institute for Molecular Studies approved the study.
Measurements of the serum FFA u concentrations were performed using the fluorescent probe ADIFAB2 (FFA Sciences LLC, San Diego, California), as described previously for patients with cardiac ischemia and MI ; however, it was modified for 96-well plate fluorometry using a Flurolog 3 spectrofluorometer with a MicroMax plate reader (Horiba Ltd., Kyoto, Japan). Serum samples were diluted to 1% (vol/vol) in 200 μl of measuring buffer in 96-well plates. Fluorescence was measured after adding ADIFAB2 (1.5 μmol/L), and the intensities were used to determine the ratio (R) of the fluorescence intensities at 550 to 457 nm, with the background subtracted. Sample FFA u concentrations (nmol/L) were calculated using FFA u = 227 (R − R o )/(0.925 − R), where R o is the ADIFAB2 fluorescence ratio in the absence of FFA, and the numerical factors were determined as described previously. All samples were measured in duplicate, yielding an average coefficient of variation of 6.5%.
FFA u quartiles were determined using all baseline FFA u values ( Table 1 ). Correlations between the FFA u level and baseline patient characteristics were performed using all cardiovascular confounders available in the limited data set. In the TIMI II, patients with renal disorders were excluded, the Killip class was not recorded, and creatine kinase was the only cardiac biomarker measured. The outcomes of death from STEMI, cardiac causes, and all-causes were determined through committee adjudication by the TIMI investigators. Statistical analyses were performed using XLSTAT (Addinsoft, New York, New York), and p ≤0.05 was considered significant.
| Q1 (n = 458) | Q2 (n = 458) | Q3 (n = 459) | Q4 (n = 459) | p Value | |
|---|---|---|---|---|---|
| FFA u (nmol/L) | 1.9 (0.09–2.6) | 3.2 (2.6–3.9) | 4.9 (3.9–6.4) | 10.2 (6.46–523) | |
| Age (yrs) | 53.9 | 53.8 | 55.3 | 55.4 | 0.008 |
| Men | 398 (87) | 389 (85) | 344 (75) | 372 (81) | <0.0001 |
| White | 398 (87) | 398 (87) | 409 (89) | 398 (87) | 0.62 |
| BMI (kg/m 2 ) | 27 (15–40) | 27 (18–46) | 27 (16–54) | 27 (17–54) | 0.55 |
| DBP (mm Hg) | 81 (42–130) | 81 (50–110) | 80.2 (40–120) | 78.2 (40–118) | 0.053 |
| SBP (mm Hg) | 130 (56–180) | 130 (60–183) | 129 (80–210) | 126 (50–190) | 0.044 |
| Creatine kinase (IU/L) | 105 (5–1,760) | 104 (12–3,590) | 94 (11–4,422) | 99 (11–3,654) | 0.080 |
| Diabetes mellitus | 41 (9) | 37 (8) | 73 (16) | 78 (17) | <0.0001 |
| Previous MI | 60 (13) | 64 (14) | 69 (15) | 73 (16) | 0.50 |
| Previous hypertension | 174 (38) | 156 (34) | 188 (41) | 179 (39) | 0.20 |
| β Blocker within 24 h | 87 (19) | 87 (19) | 78 (17) | 73 (16) | 0.68 |
Results
The baseline FFA u levels were measured in serum samples collected within 4 hours of initial symptom onset. The FFA u concentrations ranged from <1 to >500 nmol/L ( Table 1 ). This range was larger than that we had reported previously for a cohort of nominally healthy subjects whose range was 0.6 to 4.5 nmol/L (mean 1.5). The correlations of the FFA u quartiles with all cardiovascular risk factors available from the limited access data set and for which the patients with the indicated risk factors comprised ≥10% of all patients are listed in Table 1 .
Of the 1,834 patients, 187 died of all causes, 125 of cardiac causes, and 76 of STEMI ( Table 2 ). A positive correlation of death from MI with FFA u quartile was present as early as 1 day after enrollment and peaked at about 30 days after enrollment. Because most deaths within 30 days were from MI, the cardiac deaths and deaths from all causes also correlated strongly with the baseline FFA u levels. The peak (within 8 hours; Table 2 ), but not baseline ( Table 1 ), creatine kinase levels also correlated with the FFA u levels.
| Median FFA u (nmol/L) | Total | p Value | p Trend | ||||
|---|---|---|---|---|---|---|---|
| Q1 (1.9) | Q2 (3.2) | Q3 (4.9) | Q4 (10.2) | ||||
| Death from | |||||||
| MI | |||||||
| At 1 day | 3 | 7 | 11 | 12 | 33 (1.8) | 0.1 | 0.015 |
| At 7 days | 3 | 7 | 19 | 21 | 50 (2.7) | 0.0002 | <0.0001 |
| At 30 days | 4 | 10 | 21 | 29 | 64 (3.5) | <0.0001 | <0.0001 |
| At 3.8 yrs | 6 | 14 | 24 | 32 | 76 (4.1) | <0.0001 | <0.0001 |
| All cardiac causes | |||||||
| At 1 day | 3 | 7 | 11 | 12 | 33 (1.8) | 0.1 | 0.015 |
| At 7 days | 3 | 7 | 19 | 21 | 50 (2.7) | 0.0002 | <0.0001 |
| At 30 days | 5 | 11 | 21 | 29 | 66 (3.6) | <0.0001 | <0.0001 |
| At 3.8 yrs | 16 | 27 | 38 | 44 | 125 (6.9) | 0.0006 | <0.0001 |
| All causes | |||||||
| At 1 day | 3 | 8 | 13 | 13 | 37 (2.0) | 0.056 | 0.0095 |
| At 7 days | 3 | 9 | 24 | 23 | 59 (3.2) | <0.0001 | <0.0001 |
| At 30 days | 5 | 13 | 26 | 34 | 78 (4.3) | <0.0001 | <0.0001 |
| At 3.8 yrs | 29 | 38 | 57 | 63 | 187 (10) | 0.0004 | <0.0001 |
| Noncardiovascular causes at 3.8 yrs ∗ | 13 | 9 | 13 | 15 | 50 (2.7) | 0.67 | 0.530 |
| Other outcomes | |||||||
| Peak (8 h) creatine kinase (IU/L) | 1,628 | 1,957 | 2,039 | 2,156 | <0.0001 | ||
∗ An additional 12 patients died of hemorrhage during the 3.8 -year follow-up period (4 at day 1); summing all cardiac plus noncardiovascular deaths, plus 1 death without cause equaled 187.
Relative to the total TIMI II population, the FFA u levels correlated positively with female gender, age, and diabetes. Approximately twice as many women and patients with diabetes were in the upper 2 FFA u quartiles ( Table 1 ). Deaths from MI in nondiabetic women, men, and patients with diabetes increased with increasing FFA u quartile ( Table 3 ). This correlation reached significance in nondiabetic women and men but not in those with diabetes. The lack of correlation in those with diabetes was likely because of the small numbers and 2 deaths within 5 hours in those in the first quartile but no additional deaths in the first quartile during the next 3.8 years. The death rate for women and those with diabetes was almost twofold greater than that for the nondiabetic men, except for at day 1, mostly owing to the larger death rates at 30 days in the third and fourth FFA u quartiles. Using subgroup interaction analysis, the death rates in quartiles 3 and 4 were significantly (p = 0.05) higher in nondiabetic women than men but not (p = 0.07) for all those with diabetes versus those without diabetes.
| Death | FFA u | Total | p Value | p Trend | |||
|---|---|---|---|---|---|---|---|
| Q1 | Q2 | Q3 | Q4 | ||||
| Nondiabetic women (n = 283) | |||||||
| By 1 day | 0 | 1 | 1 | 3 | 5 (1.8) | 0.02 | 0.10 |
| By 7 days | 0 | 1 | 5 | 6 | 12 (4.2) | 0.08 | 0.009 |
| By 30 days | 0 | 2 | 5 | 8 | 15 (5.3) | 0.04 | 0.004 |
| By 3.8 yrs | 1 | 2 | 6 | 8 | 17 (6.0) | 0.1 | 0.06 |
| Nondiabetic men (n = 1,322) | |||||||
| By 1 day | 1 | 6 | 7 | 6 | 20 (1.5) | 0.9 | <0.022 |
| By 7 days | 1 | 6 | 9 | 10 | 26 (2.0) | <0.014 | <0.0018 |
| By 30 days | 2 | 7 | 11 | 14 | 34 (2.6) | <0.003 | <0.0003 |
| By 3.8 yrs | 3 | 10 | 12 | 17 | 42 (3.2) | <0.002 | <0.0002 |
| Diabetics (n = 229) | |||||||
| By 1 day | 2 | 0 | 3 | 3 | 8 (3.5) | 0.11 | 0.86 |
| By 7 days | 2 | 0 | 5 | 5 | 12 (5.2) | 0.44 | 0.37 |
| By 30 days | 2 | 1 | 5 | 7 | 15 (6.6) | 0.57 | 0.23 |
| By 3.8 yrs | 2 | 2 | 6 | 7 | 17 (7.4) | 0.79 | 0.32 |
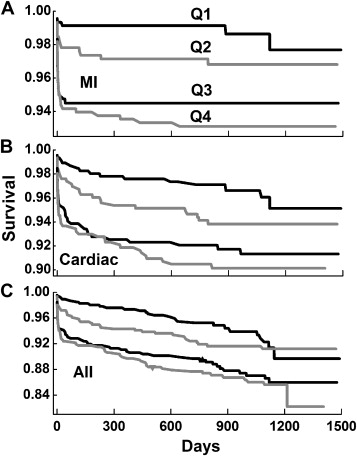
Kaplan-Meier survival curves for deaths from STEMI, all-cardiac causes, and all causes revealed striking dependencies on the FFA u quartiles ( Figure 1 ). Log-rank tests indicated that the risk of death for all 3 categories increased significantly (p <0.001) with increasing FFA u quartile. For MI, almost all deaths occurred within the first 30 days. For deaths from all causes, the survival curve revealed a similar slope after 60 days for all 4 quartiles, consistent with a lack of correlation with the FFA u concentration for noncardiac mortality ( Table 2 ). Cox proportional hazard modeling of the 3 sets of survival curves revealed hazard ratios that increased significantly with FFA u quartile relative to the first quartile and were relatively unaffected by other risk factors ( Table 4 ). The unadjusted hazard ratios for MI deaths increased from 2.3 for quartile 2 to 5.6 for quartile 4; the corresponding adjusted hazard ratios were 2.9 and 5. Except for the quartile 1 to quartile 2 increase, the hazard ratio increases with FFA u quartile were significant (p ≤0.03) for all unadjusted and adjusted analyses.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


