Previous data have indicated that carotid plaque ulceration is a strong predictor of cerebrovascular events. Standard ultrasound and color Doppler ultrasound (CDUS) scans have poor diagnostic accuracy for the detection of carotid plaque ulceration. The aim of the present prospective study was to assess the value of contrast-enhanced ultrasound (CEUS) scans for the detection of carotid plaque ulceration. The Institutional Ethics Committee approved the study protocol, and all patients provided informed consent. The patients had symptomatic stenosis of the internal carotid artery and underwent carotid computed tomographic angiography as part of their clinical evaluation. All patients underwent a CDUS examination in conjunction with CEUS. Carotid plaque ulceration was defined as the presence of ≥1 disruptions in the plaque–lumen border ≥1 × 1 mm. Carotid computed tomographic angiography was used as reference technique. The study population consisted of 20 patients (mean age 64 ± 9 years, 80% men), and 39 carotid arteries were included in the present analysis. Computed tomographic angiography demonstrated that the plaque surface was smooth in 15 (38%), irregular in 7 (18%) and ulcerated in 17 (44%) carotid arteries. The sensitivity, specificity, accuracy, positive predictive value, and negative predictive value of CDUS for the detection of ulceration was 29%, 73%, 54%, 46%, and 57%, respectively. The sensitivity, specificity, accuracy, positive predictive value, and negative predictive value of CEUS for the detection of ulceration was 88%, 59%, 72%, 63%, and 87%, respectively. CEUS had superior sensitivity and diagnostic accuracy for the assessment of carotid plaque ulceration compared with CDUS. CEUS improved the intrareader and inter-reader variability for the assessment of carotid plaque ulceration compared with CDUS. In conclusion, CEUS could be an additional method for the detection of carotid plaque ulceration. The role of CDUS for the assessment of carotid plaque ulceration seems limited.
Previous studies have demonstrated that carotid plaque ulceration is a strong predictor of cerebrovascular events. Ultrasound is the most frequently used imaging technique for the assessment of carotid atherosclerosis. It is readily available, of low cost, safe, and accurately identifies the presence of flow-limiting stenosis. Nevertheless, ultrasound, including color Doppler ultrasound (CDUS), fails to accurately identify carotid plaque ulceration. Contrast-enhanced ultrasound (CEUS) is an advanced form of ultrasound imaging using a microbubble contrast agent. CEUS provides a better delineation of the carotid lumen than does CDUS. The use of CEUS for the detection of carotid plaque ulceration has not yet been studied. The aim of the present prospective study was to assess the value of CEUS for the detection of carotid plaque ulceration in patients with symptomatic carotid atherosclerosis. Carotid computed tomographic angiography (CTA) was used as the reference technique.
Methods
The Institutional Ethics Committee approved the study protocol. All patients provided informed consent. A total of 20 consecutive patients were included in the present study. All patients had symptomatic stenosis of the internal carotid artery and underwent carotid CTA as part of their clinical evaluation. All patients also underwent a carotid CDUS examination in conjunction with CEUS. The exclusion criteria included contraindications for the use of an ultrasound contrast agent, such as unstable angina, acute cardiac failure, acute endocarditis, known right-to-left shunts, and a known allergy to microbubble contrast agents.
CDUS and CEUS were performed using a Philips iU-22 ultrasound system (Philips Medical Systems, Bothell, Washington), equipped with an L9-3 transducer. CDUS consisted of standard B-mode and color Doppler imaging and was performed using a standard scanning protocol. In brief, both left and right carotid arteries were examined with the patient in the supine position with the head supported at a 45° angle turned to the contralateral side. The common carotid artery, carotid bulb, internal carotid artery, and external carotid artery were evaluated using CDUS and pulsed wave Doppler imaging. All anatomic sites were examined from different angles of view, and each site was scanned in the cross-sectional view and longitudinal view.
After the CDUS examination, CEUS was performed using intravenous administration of SonoVue contrast agent (Bracco SpA, Milan, Italy). The contrast mode of the ultrasound system, using amplitude modulation and a mechanical index of 0.06, was used to optimize the CEUS examination. The ultrasound contrast agent was injected in 0.5-ml boluses. Each contrast agent bolus was followed by a saline flush using 2.0 ml NaCl 0.9% solution. After administration of the contrast agent, high-quality contrast images could be obtained for approximately 1 minute. The bolus injection of the contrast agent was repeated when necessary. Both carotid arteries were examined using a standard acquisition protocol, and still frames and cine clips were digitally stored for offline analysis.
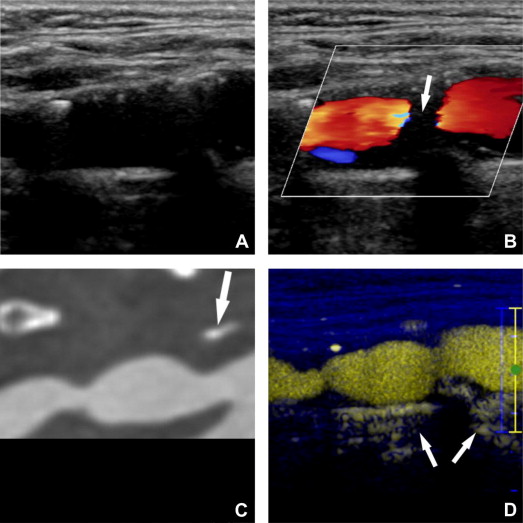
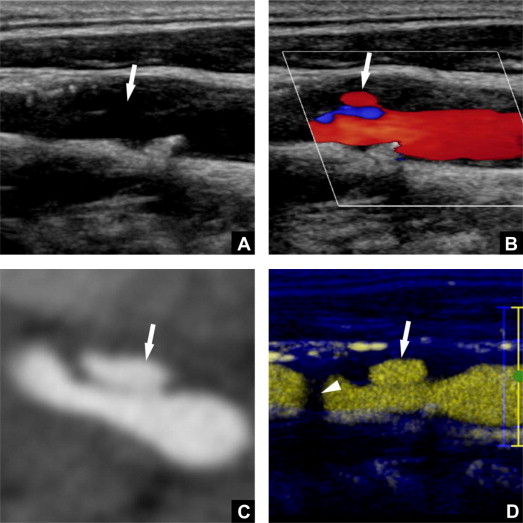
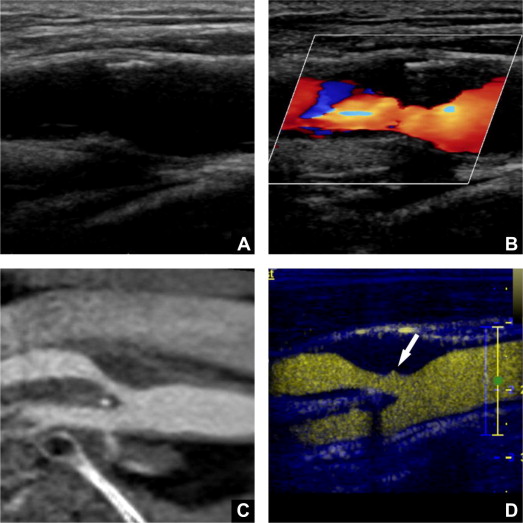
All studies were analyzed by 2 readers who were unaware of the clinical and CTA data. Discrepancies in their readings were resolved by consensus; if a consensus could not be reached, a third experienced reader was consulted. The CDUS and CEUS studies were analyzed separately. The image quality of the region of interest was scored using a 3-point scale as good, moderate, or poor image quality. The plaque border was visually scored as smooth, irregular ( Figure 1 ), or ulcerated ( Figures 2 and 3 ). Carotid plaque ulceration was defined as the presence of ≥1 disruptions of the plaque–lumen border ≥1 × 1 mm. The presence of calcification was scored using a semiquantitative grading system: 0, no calcification; 1, limited calcification; 2, moderate calcification; and 3, severe calcification. For each study, the readers indicated whether the presence of calcification hindered the evaluation of the plaque surface morphology.
CTA was performed using a 128-slice, multidetector CT system (Definition AS+ or Definition flash [1 patient], Siemens Medical Solutions, Forchheim, Germany) using a contrast-enhanced CTA protocol (120 kVp, 180 mA, collimation 64 × 2 × 0.6 mm, pitch <1). The scan range extended from the ascending aorta to the intracranial circulation (3 cm above the sella turcica). Of the 20 patients, 19 received 80 ml of contrast agent (320 mg/ml iodixanol, Visipaque, Amersham Health, Little Chalfont, United Kingdom), followed by 45-ml saline bolus chaser, both at an injection rate of 5 ml/s. One patient received 60 ml of contrast agent, followed by a 45-ml saline bolus chaser, both at an injection rate of 4 ml/s. Real-time bolus tracking at the level of the ascending aorta was used to synchronize the passage of the contrast agent and data acquisition. Image reconstructions were made with a field of view of 120 to 170 mm, matrix size 512 × 512, slice thickness 1.0 mm, increment 0.6 mm, and an intermediate reconstruction algorithm.
All CTA studies were evaluated with the reviewers unaware of the clinical and ultrasound data. A 2-dimensional axial image viewer was used to assess the image quality and degree of stenosis of both carotid arteries. The image quality of the region of interest was scored using a 3-point scale as good, moderate, or poor image quality. The degree of stenosis was calculated using the North American Symptomatic Carotid Endarterectomy Trial (NASCET) criteria perpendicular to the central lumen line. Dedicated 3-dimensional analysis software with multiplanar reformatting was used to evaluate the plaque surface in the oblique, coronal, and sagittal plane. The plaque surface of all carotid arteries was independently evaluated by 2 readers. Discrepancies in their evaluation were solved by consensus; if consensus could not be reached, a third experienced reader was consulted. The CTA and ultrasound studies were analyzed by different readers. The surface of the plaque was scored as smooth, irregular, or ulcerated. Carotid plaque ulceration was defined as the presence of contrast extending beyond the vascular lumen ≥1 mm in ≥2 planes. The calcium volume was measured from 3 cm proximal to 3 cm distal of the flow divider using semiautomated quantification software. A threshold of 600 Hounsfield units was used to differentiate calcium from contrast.
Statistical analyses were performed using the Statistical Package for Social Sciences for Windows, version 17.0 (SPSS, Chicago, Illinois). Continuous variables are reported as the mean ± SD or median and interquartile range. Categorical variables are expressed as numbers and percentages. The CDUS and CEUS studies of the right and left carotid artery were analyzed independently, with the corresponding CTA study as the reference technique. The measurements of accuracy (sensitivity, specificity, accuracy, positive predictive value, and negative predictive value) were calculated. Differences in diagnostic accuracy were compared using McNemar’s test. The CTA determined calcium volume and ultrasound calcium scores were compared using Spearman’s rank correlation. The inter-reader and intrareader reproducibility was assessed using weighted κ statistics. p Values <0.05 were considered statistically significant.
Results
The clinical characteristics of the study population (mean age 64 ± 9 years, 80% men) are listed in Table 1 . All CDUS, CEUS, and CTA studies were performed without adverse reactions. One patient had previously undergone right-sided endarterectomy; this carotid artery was excluded from the analysis, resulting in 39 carotid arteries for the present analysis.
| Variable | Value |
|---|---|
| Men | 16 (80) |
| Age (yrs) | 64 ± 9 |
| Body mass index (kg/m 2 ) | 29 ± 6 |
| Hypertension | 10 (50) |
| Diabetes mellitus | 5 (25) |
| Smoker | 9 (45) |
| Quit smoking | 6 (30) |
| Dyslipidemia | 7 (35) |
| Coronary artery bypass grafting | 2 (10) |
| Myocardial infarction | 1 (5) |
| Amaurosis fugax | 5 (25) |
| Transient ischemic attack | 8 (40) |
| Ischemic stroke | 5 (25) |
| Retinal infarction | 1 (5) |
| Pulsatile tinnitus | 1 (5) |
| Platelet aggregation inhibitor use | 19 (95) |
| β-Blocker therapy | 12 (60) |
| Statin therapy | 19 (95) |
The image quality of the CDUS studies was good in 31 (79%), moderate in 6 (15%), and poor in 2 (5%) carotid arteries. CEUS resulted in improved image quality, with 37 (95%) studies of good, 2 (5%) of moderate, and 0 of poor quality. None of the ultrasound studies were judged to be uninterpretable. The CTA image quality was good in 37 (95%) and moderate in 2 (5%) arteries. No CTA scan was judged to be uninterpretable.
CTA demonstrated that the plaque surface was smooth in 15 (38%), irregular in 7 (18%), and ulcerated in 17 (44%) carotid arteries ( Table 2 ). The performance characteristics of CDUS for the evaluation of the carotid plaque surface are listed in Table 3 . CDUS revealed 5 of 17 ulcerations (29%) identified at CTA, with 6 additional ulcerations detected that could not be confirmed. This resulted in a poor agreement between CDUS and CTA (κ = 0.19, 95% confidence interval [CI] 0.00 to 0.42).
| Variable | Value |
|---|---|
| Mean stenosis (NASCET [%]) | 43 ± 24 |
| <50% NASCET stenosis | 18 (46) |
| 50–69% NASCET stenosis | 17 (44) |
| ≥70% NASCET stenosis | 4 (10) |
| Plaque surface morphology | |
| Ulcerated | 17 (44) |
| Irregular | 7 (18) |
| Smooth | 15 (38) |
| Presence of calcium | 35 (90) |
| Calcium volume (mm 3 ) | |
| Median | 35.2 |
| Interquartile range | 7.1–127.4 |
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


