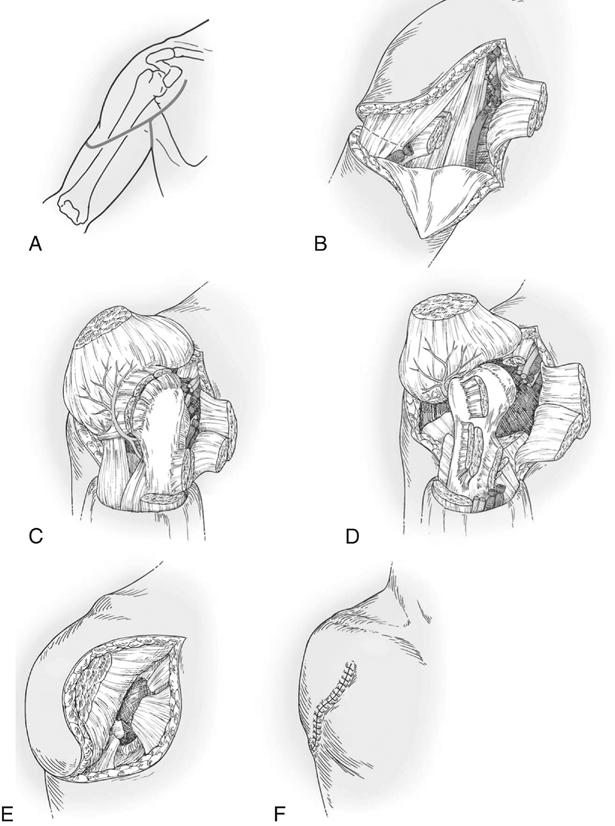
Once the site is opened through the skin, the cephalic vein is identified and ligated. The deltoid is retracted laterally, and the pectoralis major is incised near its insertion and retracted medially. The axillary artery and vein and the thoracoacromial artery are then isolated and ligated before transection. The radial, musculocutaneous, ulnar, and median nerves are isolated, drawn into the field, ligated, and transected as proximally as possible. Next, the insertions of the coracobrachialis, teres minor and teres major, the deltoid, and the origin of the triceps are incised, followed by the subscapularis and the anterior joint capsule. Once the humerus is dissected free, the limb may be removed. The deltoid is then sutured inferior to the glenoid to cover the open wound, and the skin is closed (Figure 1).
Upper Extremity Amputations
Shoulder Disarticulation
![]()
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


Thoracic Key
Fastest Thoracic Insight Engine