Chapter 26 Univentricular Heart
In 1858, Thomas Peacock described hearts in which “The auricular sinuses are separated by a more or less complete septum, and there are generally two auriculo-ventricular apertures, while the ventricle is either wholly undivided or presents only a very rudimentary septum. The arteries which are given off are usually two in number—an aorta and a pulmonary artery.”1
These cases correspond to hearts that consist of two auricles and only one ventricle. A case described by Chemineau in 1699 appears to have been of this description.2
The univentricular heart is unique in its complexity and scope and has sparked intense debate about terminology and embryology.2 Nearly a century and a half after Peacock’s1 description, there is still no consensus about the terminology for hearts with one ventricle.3–6 Single ventricle and univentricular are synonymous (single = uni = one), so these terms are interchangeable and are appropriate when two atria are related entirely or almost entirely to one ventricular compartment that qualifies on purely morphologic grounds as a left, right, or indeterminate ventricle.
Univentricular atrioventricular connection or double inlet ventricle is characterized according to gross morphologic features of the ventricular mass and according to the atrioventricular connections to that mass.4,5,7 Clinically undetectable and clinically irrelevant developmental considerations are important to the morphologist4 but should not determine clinical terminology. It is best to avoid inherently contradictory terms such as ventricular septal defect8 and interventricular communication that imply the presence of two anatomically definitive ventricles divided by a septum. To say that a ventricular septal defect exists in a heart with a single ventricle and “not a trace of an inter-ventricular septum”1 strikes most readers as contradictory irrespective of theoretic arguments to the contrary. The term “functionally” univentricular as applied to the hypoplastic left heart should be regarded as a separate category.9 In this chapter, univentricular and single ventricle refer to hearts in which one ventricular chamber receives the entire flow from the right atrium and the left atrium, both of which together with the entire atrioventricular junction are related to the single ventricle.
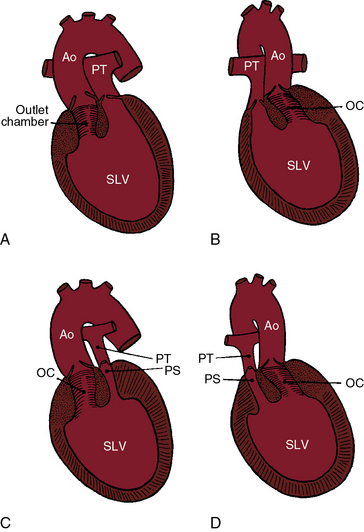
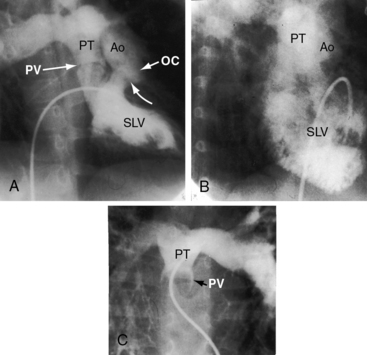
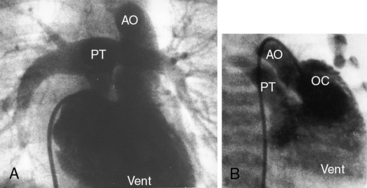
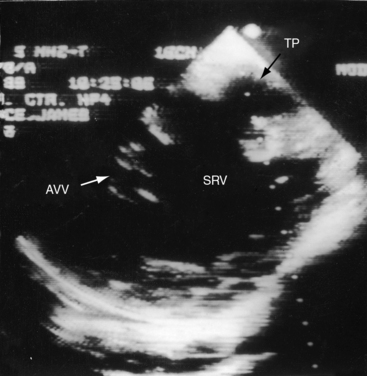
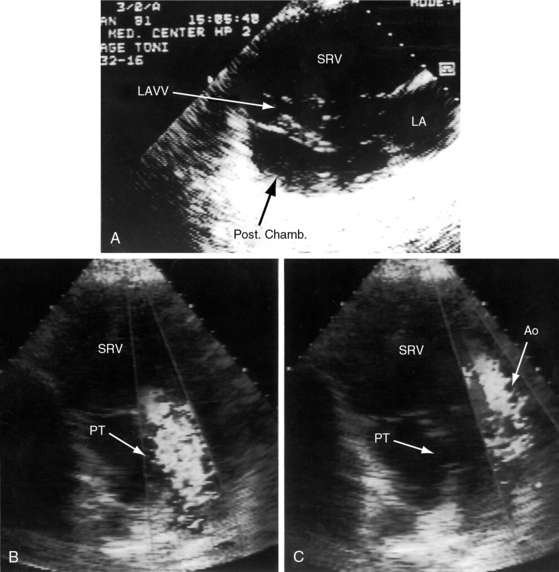
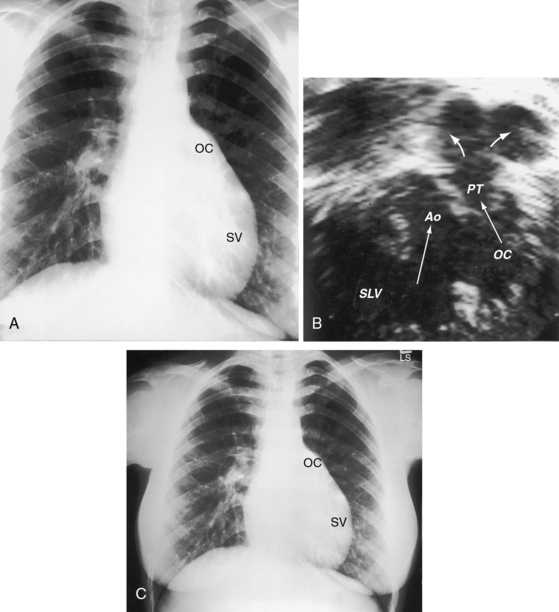
In 80% to 90% of cases, the ventricular chamber that receives the atrioventricular connections is a morphologic left ventricle that incorporates at its base an outlet chamber that is devoid of a sinus or inlet component, that is devoid or virtually devoid of trabeculae, and that is remote from the crux of the heart (Figures 26-1 through 26-4).7 In 10% to 25% of cases, the ventricular chamber that receives the atrioventricular connections has right ventricular morphologic features and incorporates within its mass a rudimentary compartment—a left ventricular remnant or trabecular pouch—that varies in size from well-formed to microscopic (see Figures 26-31 and 26-32).3,7 The trabecular pouch occupies a posterior, inferior, or lateral position within the ventricular mass and may or may not communicate with the cavity. In less than 10% of cases, the univentricular heart has indeterminate morphologic features and incorporates neither an outlet chamber nor a trabecular pouch. Because an indeterminate ventricle does not contain remnants of either a rudimentary morphologic right ventricle or a rudimentary morphologic left ventricle, the term univentricular heart or single ventricle is unassailable on morphologic grounds.
The atrioventricular connections that guard the inlet of a univentricular heart consist of either two separate valves, one patent valve with atresia of the other valve, or a common atrioventricular valve.10,11 It is customary to refer to right atrioventricular or left atrioventricular valves, rather than tricuspid and mitral valves, because tricuspid and mitral morphologic features are not necessarily evident.8 An atrioventricular (AV) valve is likely to be abnormal when it is concordant with the ventricular loop (right AV valve with noninverted outlet chamber, left AV valve with inverted outlet chamber).8,10,12 When the outlet chamber is inverted, the left AV valve tends to be stenotic, and when the outlet chamber is noninverted, the right atrioventricular valve tends to be incompetent.8 A common atrioventricular valve is usually equipped with four leaflets,11 and right atrial isomerism is the usual pattern.11 Straddling of a right or a left AV valve or a common AV valve refers to attachments of tensor apparatus to both sides of an outlet foramen or to both sides of a trabecular pouch.7,8,10,12,13
In univentricular hearts that are morphologically left ventricular, the outlet chamber is anterosuperior and either to the right or left of midline. Noninverted applies to a right anterosuperior position of the outlet chamber, and inverted applies to a left anterosuperior position (see Figures 26-1 through 26-4). The outlet chamber is either smooth-walled and devoid of trabeculations (see Figure 26-4) or contains scanty ill-defined trabeculations (see previous). The aorta arises discordantly from the outlet chamber, and the pulmonary trunk arises discordantly from the single morphologic left ventricle (see Figures 26-1 through 26-4),7 so the great arteries are transposed (see Chapter 27).
In 1824, Andrew Fernando Holmes, who would later become the first Dean of the Medical Faculty at McGill University, published autopsy observations on a 21-year-old man who died with chronic cyanosis and congestive failure. In the uncommon Holmes heart, the aorta arises concordantly from the morphologic left ventricle and the pulmonary trunk arises concordantly from the outlet chamber (see Figure 26-20). William Osler urged Maude Abbott to republish the case, which was included in her seminal atlas of 1936.14,15 Andrew Fernando Holmes was Canadian, but his 1824 publication on single ventricle was published in a Scottish journal16 because he trained at the University of Edinburgh. Rarely, the outlet chamber gives rise to both great arteries, to neither great artery, or to a common arterial trunk. In univentricular hearts characterized by a single morphologic right ventricle, both great arteries originate from the right ventricle, an arrangement that is a form of double outlet right ventricle (see Chapter 19). Occasionally, the pulmonary trunk originates concordantly from a single right ventricle, and the aorta originates concordantly from the trabecular pouch, which is a left ventricular remnant. A morphologically indeterminate single ventricle incorporates neither an outlet chamber nor a trabecular pouch (see previous), so both great arteries necessarily arise from the indeterminate single ventricle.
The orifice that joins a single left ventricle to an outlet chamber has been variously referred to as a bulboventricular foramen, a ventricular septal defect,8 and an interventricular communication. Bulboventricular foramen assumes that the embryologic foramen is the communication that exists in the univentricular heart, which is not necessarily the case. The terms ventricular septal defect and interventricular communication are discouraged as inherently contradictory (see previous). Outlet foramen is a simple descriptive term that is used herein to refer to the orifice between a single left ventricle and the outlet chamber. A restrictive outlet foramen is a form of subaortic stenosis that can be acquired8 or present at birth7 and tends to coexist with coarctation of the aorta.7
When the pulmonary trunk originates from a single morphologic left ventricle, the accompanying pulmonary stenosis is either subpulmonary or in a bicuspid pulmonary valve (see Figures 26-1, 26-2C, and 26-3).7 Pulmonary stenosis is a feature of the Holmes heart (see Figure 26-20)16 and usually results from obstruction of the outlet foramen of the concordant subpulmonary outlet chamber.14,15,17,18 The degree of stenosis ranges from mild to severe (see Figures 26-2 and 26-3) to atresia (Figure 26-5), a spectrum recognized by Peacock:
“The case of Fleischmann differed in some degree … as though the heart consisted of three cavities, the ventricle only gave rise to one vessel, the orifice of the pulmonary artery being impervious. The child had lived twenty one weeks.”1
Coronary artery origins in univentricular hearts of left ventricular morphology depend on the location of the outlet chamber (see Chapters 6 and 32). A major branch of each coronary artery usually outlines or delimits the surface boundaries of the outlet chamber.
The morphogenesis of univentricular hearts is believed to reside in an abnormality of the ventricular trabecular components of the developing heart.7,19 The left ventricular trabecular component is normally derived from the inlet portion of the embryonic heart tube, and the right ventricular trabecular component is derived from the outlet portion. As the ventricular mass develops, the atrioventricular junction is shared between the left ventricular trabecular component and the right ventricular trabecular component. When the atrioventricular junction retains its connection to the left ventricular trabecular component, the result is double inlet to a morphologic left ventricle. When the atrioventricular junction retains its connection to the right ventricular trabecular component, the result is double inlet to a morphologic right ventricle. When right and left ventricular trabecular components fail to develop, the result is double inlet to an indeterminate ventricle.
The physiologic derangements associated with univentricular hearts are related to six variables: (1) the inherent mechanics of a single ventricle20–23; (2) the mechanics of a morphologic right ventricle versus a morphologic left ventricle24; (3) the morphology and functional state of the atrioventricular valves that guard the inlet to a single ventricle; (4) the degree of mixing within the single ventricle; (5) the pulmonary vascular resistance; and (6) the presence and degree of pulmonary stenosis or subaortic stenosis.18,25
In hearts with two ventricles, each ventricle augments the function of the other ventricle.20,21 Ventricular-ventricular interaction is an integral part of cardiac mechanics and results from coupling of the two ventricles through the interventricular septum and through an anatomic continuum that joins the mural myocardium of the two ventricles.20,21 Ventricular interdependence does not occur unless a right ventricle contributes to left ventricular function and a left ventricle contributes to right ventricular function. Accordingly, ventricular interdependence does not exist in univentricular hearts. The result is abnormal systolic and diastolic function, irrespective of the morphology of the single ventricle.26,27 Because a single ventricle is the pump that serves both the systemic and the pulmonary circulations, the volume handled by a univentricular heart is increased and provokes an adaptive increase in ventricular mass.26–28 In univentricular hearts of right ventricular morphology, the indices that reflect an adaptive increase in ventricular mass are significantly reduced, including mass per se, wall thickness, ratio of wall thickness to transverse ventricular diameter, and ratio of ventricular mass to end-diastolic volume.28 Inadequate mass relative to chamber volume reflects poor adaptation of univentricular hearts of right ventricular morphology.24,28
The physiology of the circulation in univentricular hearts is materially influenced by atrioventricular valve structure and function. Incompetence, stenosis, or atresia of an atrioventricular valve affects flow into the single ventricle and modifies its loading conditions. Atrioventricular valve regurgitation adds to the volume overload of the single ventricle. Atresia of the right or left atrioventricular valve results in a single inlet that does not disturb the circulation, provided there is free access to the single ventricle via a nonrestrictive interatrial communication and across the contralateral atrioventricular valve. However, when the right atrioventricular valve is atretic and the interatrial communication is restrictive, the right atrium is obstructed.29 Similarly, the left atrium is obstructed when the left atrioventricular valve is atretic and the interatrial communication is restrictive.
Right atrial venous blood and left atrial arterialized blood remain remarkably separate within the single ventricular chamber.25 Separation of the streams is greater when pulmonary resistance is low and when the outlet chamber is inverted.25 Unoxygenated blood from the systemic venous atrium selectively finds its way into the pulmonary trunk, and oxygenated blood from the pulmonary venous atrium selectively finds its way into the aorta. Subaortic stenosis diverts even more blood into the pulmonary circulation, so cyanosis is mild and occasionally absent. However, the benefits of increased pulmonary blood flow are achieved at the price of volume overload of the single ventricle.
Pulmonary vascular disease and pulmonary stenosis curtail pulmonary blood flow and adversely affect streaming within the single ventricle. When pulmonary stenosis or pulmonary vascular disease are severe, cyanosis is conspicuous because a smaller volume of oxygenated blood reaches the left atrium and because there is greater mixing of unoxygenated and oxygenated blood within the single ventricle.18
History
The male:female ratio in univentricular hearts is between 2:1 and 4:1.30 Recurrence in siblings is rare.31 Neonates or infants come to attention because of congestive heart failure, cyanosis, or a murmur. The type of presentation and the survival patterns depend on the pulmonary vascular resistance, the presence and degree of pulmonary stenosis, the morphology of the single ventricle, and the presence and degree of subaortic stenosis. Fifty percent of patients with univentricular hearts of left ventricular morphology die within 14 years, with an annual attrition rate of 4.8%.32 Fifty percent of patients with univentricular hearts of right ventricular morphology are dead within 4 years.32
Infants with increased pulmonary blood flow present with congestive heart failure, mild cyanosis, and poor growth and development.18 When subaortic stenosis augments already excessive pulmonary blood flow, congestive failure is refractory. Pulmonary vascular resistance seldom achieves satisfactory regulation of pulmonary flow. The oldest reported survivor with a single morphologic left ventricle and pulmonary vascular disease was a 59-year-old man.33 An exceptional case similar, if not identical, to the 24-year-old man (referred to in Figure 26-18), was described by Peacock1 in a 24-year-old man.
< div class='tao-gold-member'>
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


