Tberculosis clinical manifestations
Pulmonary Presentations
Pulmonary Infection or Classic Primary Complex
This presentation is the most common one (90%) and appears in a self-limited form. By having nonspecific respiratory symptoms such as cough and secretions, often it goes unnoticed and is confused with a banal viral infection. Phlyctenular keratoconjunctivitis and nodular erythema are infrequent signs. Small children and adolescents tend to be more symptomatic. Chest X-ray may show the classic radiological image of hilar adenopathy and, less frequently, a figure resembling a loaded barbell, which denotes Ghon’s primary complex. Radiological signs tend to take 6–12 months to disappear, although calcifications may develop in the future.
Patients are diagnosed through a positive PPD test or a boosted PPD test, in the context of a contact study of a bacilliferous case. In these cases, it is important to implement a treatment, because the probability of developing the disease with pulmonary or extrapulmonary presentations increases during the first 2 years after the primary infection.
Pulmonary Disease: Progressive Pulmonary Presentations
Nowadays, this presentation is highly exceptional. The development of this clinical manifestation is basically determined by the immunity of the host, so it increases in children younger than 2 years old, children with a poor nutritional state, those who did not receive the BCG vaccine, or are HIV positive, as well as those who are exposed to close contact with bacilliferous sick patients. The pulmonary manifestation is very similar to the clinical presentation of any pneumonia: coughing, fever, expectoration, and dyspnea, and the differential diagnosis includes the suspicion of this possibility when there is no adequate clinical response. When there is a parenchymal progression to cavitary presentations, caseous pneumonia, or primary phthisis, the following symptoms can also be observed: asthenia, adynamia, night sweats, weight loss, and hemoptysis.
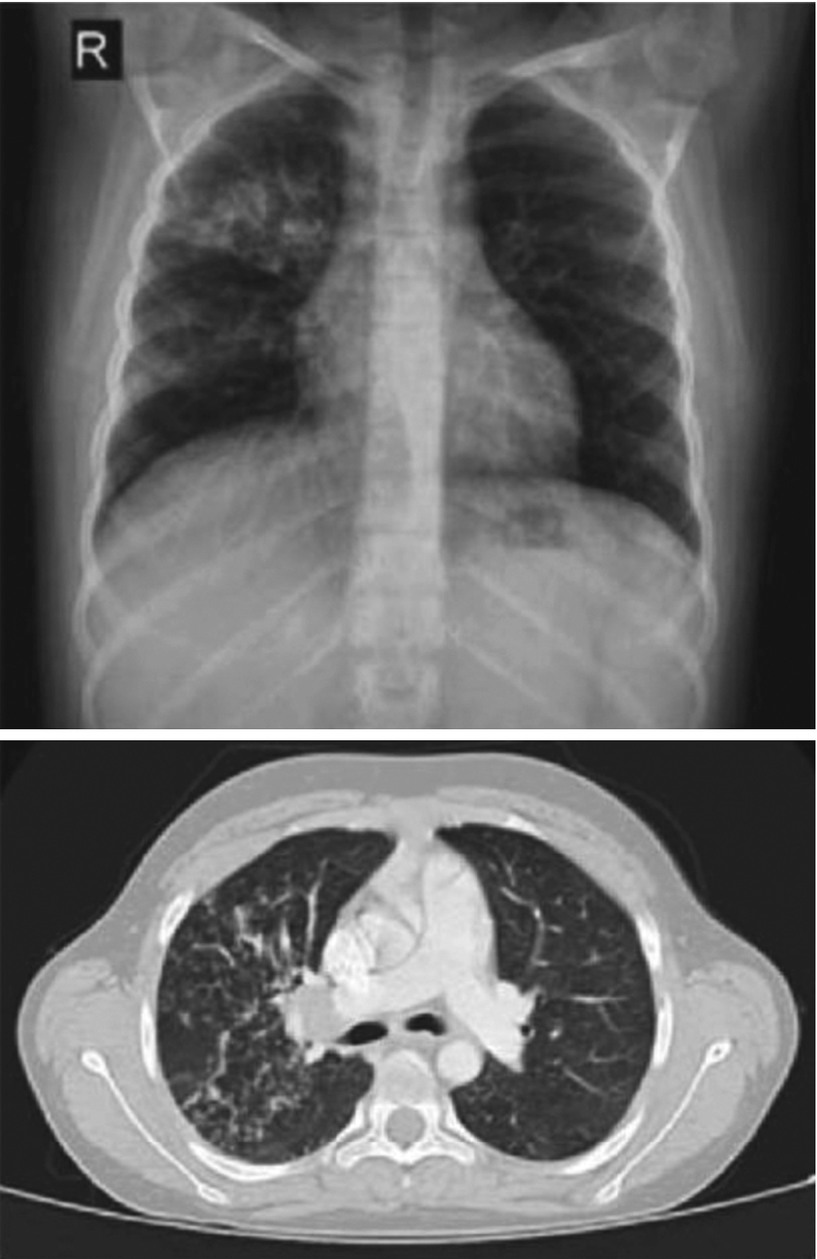
Tuberculosis with bronchogenic dissemination in 10-year-old patient with an HIV infection responding poorly to antiretroviral therapy. Anteroposterior (AP) chest X-ray shows primary alveoli compromise in right upper lobe (RUL) (a) and during computed tomorgraphy (CT) (b), where bronchial invasion is observed in RUL bronchus and subsequent lumen obstruction
Adult-Type Tuberculosis

Adult-type tuberculosis . AP radiography of 14-year-old adolescent who presented clinically with a prolonged fever and coughing with bacilliferous expectoration. Condensation in RUL is observed, secondary to alveolar compromise and atelectasis of the same zone, probably caused by lymph node compression of the corresponding bronchus
Tuberculous Adenitis
Tuberculous adenitis is the most frequent extrapulmonary presentation. It usually presents as a localized adenopathy on a lymph node or lymph pack. It can involve any lymph group, but it usually appears on the head and neck.
Adenopathy can cause a subacute presentation with mild general symptomatology or none. During the examination, the adenopathy is mobile, painless, and without erythema. If it is not treated, it increases in size and a caseous necrosis appears. In this stage, the adenopathy acquires a typical erythema tone, with a fluid texture in the centre. If this adenopathy breaks, it may cause a skin fistula or scrofula, which chronically leaks. Pulmonary compromise must be ruled out for these patients. Differential diagnoses include lymphoma and certain infectious causes, so a biopsy is fundamental for making a definitive diagnosis.
Others
Patients can present with osteoarticular, renal, genitourinary, abdominal, adrenal, parotid, ocular, and skin compromise. However, these extrathoracic presentations of tuberculosis are infrequent.
Disseminated Presentations
Disseminated presentations are serious and are characterized by a high mortality rate. They can be clinically present in three ways, depending on the immunological state of the patient and the number of bacilli that enter the bloodstream.
Miliary Tuberculosis
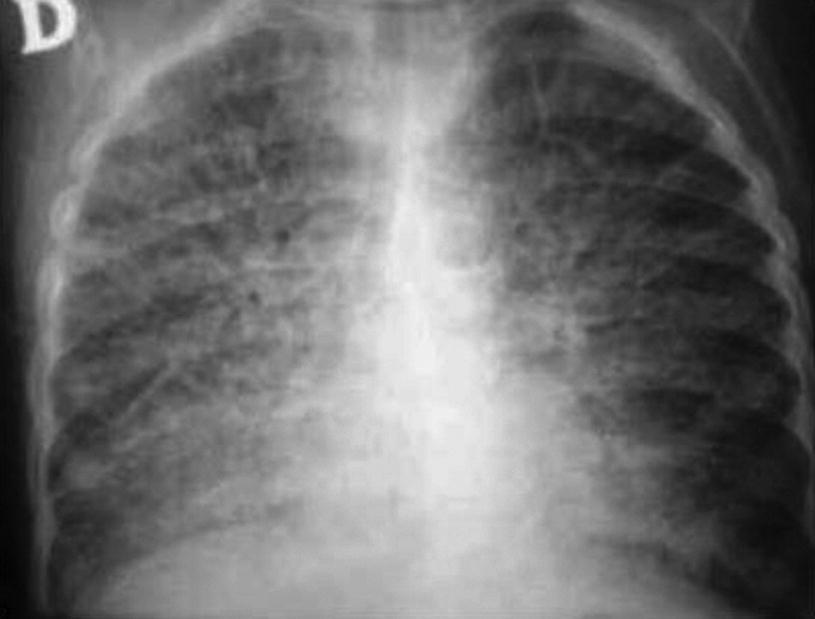
Miliary tuberculosis . AP chest X-ray of an infant with no BCG vaccine and intrafamilial contact with an adult with bacilliferous tuberculosis. Diffuse bilateral granular compromise can be observed, consistent with miliary tuberculosis
Tuberculous Meningitis
This presentation is a meningoencephalitis that mostly compromises the base of the brain and the circle of Willis. Three developmental stages can be identified, which progress during 1 to 2 weeks. In infants and small children, progression can be faster, lasting only a few days. During stage 1, nonspecific signs are predominant, including fever, lack of energy, irritability, vomiting, constipation, and delays in psychomotor development. During stage 2, an intense headache appears, as well as explosive vomiting, disorientation, and seizures. In this stage, physical examination shows meningeal signs, compromise of the cranial pairs, focal neurological signs, or hemiparesis and endocranial hypertension. Stage 3 is the most serious one, as patients display severe consciousness impairment, which ranges from stupor to coma, hemiplegia, or tetraplegia. Severe endocranial hypertension, besides decerebrate or decorticate posture, can also be observed. These patients tend to have a negative PPD test, with thorax chest X-ray revealing parenchymal compromise. Computerized tomography (CT) shows several brain areas affected by strokes and infarctions, although in some cases tuberculomas may also be observed in the cerebral parenchyma. Diagnosis is based on alterations of the cerebrospinal fluid (CSF), which is characteristically clear and low in glucose. Cytochemical analysis also shows a minor presence of chloride, a high protein level, and a slight increase in predominantly mononuclear cells . Koch’s culture, amplification methods, and adenosine deaminase (ADA) in the CSF are useful.
Connatal Tuberculosis
Connatal tuberculosis is fortunately a rare disease. It has a very high mortality rate, even when treated. It is sanguineously transmitted through the umbilical cord or through amniotic fluid aspiration during childbirth. Symptoms include respiratory failure, hepatosplenomegaly, lymphadenopathies, fever, abdominal distension, lethargy, and irritability. Skin lesions, jaundice, seizures, otorrhea, and diarrhea are seen less frequently. Some newborns present with severe septic shock.
Diagnostic Approach
Tuberculosis diagnosis in children is still a major challenge. In spite of numerous studies aimed at developing new techniques or improving on traditional ones, especially those associated with HIV infection, these techniques are not within the reach of the general population; therefore, treatment onset is frequently delayed.
- 1.
Children exposed to a bacilliferous patient.
- 2.
Children with an unresolved pneumonia, which does not respond to normal antimicrobial treatment, or with persistent signs in images.
- 3.
Children with an adult-type presentation and compatible clinical findings.
The process begins with chest X-ray, both projections (anteroposterior and lateral), PPD testing, and expectoration bacilloscopy. Thorax radiography will show different images depending on the tuberculosis presentation affecting the patient. Complementary imaging with a computerized axial tomography scan is recommended when diagnosis is uncertain.
There are tests showing immune response to Koch’s bacillus:
PPD Testing
The PPD test (protein purified derivative) is a protein concentrate of Koch’s bacillus, Calmette–Guérin (BCG), and nontuberculous mycobacteria. The PPD test is highly sensitive but nonspecific for Mycobacterium tuberculosis infection. The test consists of 2–10 U of this concentrate delivered intradermally in the external radial side of the left forearm. Subsequently, the cellular immunity response to PPD inoculation is measured. The test uses a hypersensitive delayed response, the value of which peaks at 72 h. At this point, the extent of the transverse induration is measured (pencil test). Internationally, a PPD test is considered positive when it has an induration area equivalent to or greater than 10 mm. In children younger than 4 years old, with malnutrition, immunosuppression (HIV infection), or without BCG vaccine, a test is considered positive if induration reaches or surpasses 5 mm. A tuberculous boost is defined as an induration increase greater or equal to 10 mm with a difference greater than 6 mm, which happens in 3-month intervals (up to 2 years). This reaction is compatible with a recent infection. The PPD test can yield a “false negative” after a viral infection, live virus vaccination, immunosuppression, and in severe tuberculosis presentations, especially for the most widespread forms: 5% to 10% of tuberculous diseases yield a negative PPD test.
PPD test interpretation is difficult and may lead to confusion, particularly in countries with high BCG vaccine coverage. The PPD test is useful for diagnosing double tuberculous infections in countries with a low endemic rate of Mycobacterium tuberculosis, low infection incidence for nontuberculous mycobacteria, and high BCG vaccine coverage.
IGRAS
Bacteriological study. Mycobacterium tuberculosis must be identified, which is especially difficult in children, because their lesions have a low bacillus count and they are usually poorly connected to the central airway.
Bacilloscopy requires at least 5000 BK/ml (two samples) to yield a positive result. A Ziehl–Neelsen stain is used, which requires a microscope with 1000× or greater magnification, and 10–15 min of exposure; alternatively, it is possible to use a fluorophore stain, which requires a 400× reduction in the magnification, and takes 2–3 min of exposure. WHO recommends the latter technique.
Culture requires 10 BK/ml to get a positive result and is the gold standard for diagnosis. In children it is rarely positive, except for the cases in which there are excavated lesions communicating with the central airway. Löwenstein–Jensen culture requires from 3 to 6 weeks, plus 3 additional weeks when resistance is suspected. This is a slow process, but it provides a better identification of Koch’s bacillus and drug resistance. This medium is available in regional laboratories throughout our country. The liquid medium technique takes from 1 to 3 weeks and relies on a continuous automated reading of bacterial growth, which affords greater sensitivity. It has a higher contamination rate, although it is difficult to identify the morphology of the colonies. There are also nonradiometric cultures, such as MGIT (Mycobacteria Growth Indicator Tube), the BACTEC9000MB system, and ESP Culture System II Myco, available in central laboratories.
Samples for bacteriological studies rarely come from the expectorations of sick children. In these cases, it is recommended to obtain samples by sputum induction, using a nebulized hypertonic saline solution, or aspiration of gastric content (three samples). The output of this sample is up to 30% in children, even for immunosuppressed patients with extrapulmonary tuberculosis. If the sample cannot be obtained with the aforementioned techniques, a bronchoalveolar lavage can be performed through bronchoscopy.
Amplification technique for nucleic acids. These techniques can be considered in patients under suspicion of resistance to anti-tuberculosis drugs. They have a high sensitivity (96%) and specificity (85–95%) for positive bacilloscopy samples, so they can rapidly detect a few copies of nucleic acid. They do not need to be performed in a high security laboratory (level 3), and the newest techniques also detect drug resistance and identify specific microbacteria. Nevertheless, they are not too sensitive (66%) for negative bacilloscopy samples, which is the most common situation in children, and they are not available in higher prevalence areas, where they are most needed.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


