Many treatments are available for patients with cardiovascular disease. The dramatic ones, such as heart transplantation and artificial heart insertion, have received a lot of publicity. However, some more commonly used treatment measures include:
drug therapy
surgery
balloon catheter treatments
defibrillation
synchronized cardioversion
pacemaker insertion.
DRUG THERAPY
Types of drugs used to improve cardiovascular function include:
cardiac glycosides and phosphodiesterase (PDE) inhibitors
antiarrhythmics
antianginals
antihypertensives
diuretics
adrenergics
beta-adrenergic receptor blockers
antilipemics.
Cardiac glycosides and PDE inhibitors
Cardiac glycosides and PDE inhibitors increase the force of the heart’s contractions. Increasing the force of contractions is known as a positive inotropic effect, so these drugs are also called inotropic drugs (affecting the force or energy of muscular contractions). (See Understanding cardiac glycosides and PDE inhibitors.)
UNDERSTANDING CARDIAC GLYCOSIDES AND PDE INHIBITORS
Cardiac glycosides and phosphodiesterase (PDE) inhibitors have a positive inotropic effect on the heart, meaning they increase the force of contraction. Use this table to learn about the indications, adverse reactions, and nursing considerations associated with these drugs.
If immediate effects are required (as with a supraventricular arrhythmia), a loading dose of digoxin is required.
Check apical pulse for 1 minute before administration; withhold drug and report pulse less than 60 beats/minute.
Therapeutic levels are 0.5 to 2 ng/ml.
PDE INHIBITORS
Inamrinone, milrinone (Primacor)
Heart failure refractory to digoxin, diuretics, and vasodilators
Arrhythmias
Nausea
Vomiting
Headache
Fever
Chest pain
Hypokalemia
Thrombocy-topenia
These drugs are contraindicated in patients in the acute phase of myocardial infarction (MI) and after an MI.
Serum potassium levels should be within normal limits before and during therapy.
Cardiac glycosides, such as digoxin (Lanoxin), also slow the heart rate (called a negative chronotropic effect) and slow electrical impulse conduction through the atrioventricular (AV) node (called a negative dromotropic effect).
PDE inhibitors, such as inamrinone and milrinone (Primacor), are typically used for short-term management of heart failure or long-term management in patients awaiting heart transplant surgery. PDE inhibitors improve cardiac output by strengthening contractions. These drugs are thought to help move calcium into the cardiac cell or to increase calcium storage in the sarcoplasmic reticulum. By directly relaxing vascular smooth muscle, they also decrease peripheral vascular resistance (afterload) and the amount of blood returning to the heart (preload).
Antiarrhythmics
Antiarrhythmics are used to treat arrhythmias, which are disturbances of the normal heart rhythm. (See Understanding antiarrhythmics.)
Unfortunately, many antiarrhythmics can worsen or cause arrhythmias, too. In any case, the benefits of antiarrhythmic therapy need to be weighed against its risks.
Antiarrhythmics are categorized into four major classes: I (which includes IA, IB, and IC), II, III, and IV. The mechanisms of action of antiarrhythmics vary widely, and a few drugs exhibit properties common to more than one class. One drug, adenosine (Adenocard), doesn’t fall into any of these classes.
CLASS I ANTIARRHYTHMICS
Class I antiarrhythmics are sodium channel blockers. This is the largest group of antiarrhythmic drugs. Class I drugs are commonly subdivided into classes IA, IB, and IC. With the development of many newer drugs, the use of this class of antiarrhythmics is decreasing.
Class IA antiarrhythmics
Class IA antiarrhythmics control arrhythmias by altering the myocardial cell membrane and interfering with autonomic nervous system control of pacemaker cells. Class IA antiarrhythmics include:
disopyramide (Norpace)
procainamide (Procanbid)
quinidine sulfate (Quinidex)
quinidine gluconate (Quinaglute).
Class IA antiarrhythmics also block parasympathetic stimulation of the sinoatrial (SA) and AV nodes. Because stimulation of the parasympathetic nervous system causes the heart rate to slow down, drugs that block the parasympathetic nervous system increase the AV node’s conduction rate.
This increase in the conduction rate can produce dangerous increases in the ventricular heart rate if rapid atrial activity is present, as in a patient with atrial fibrillation. In turn, the increased ventricular heart rate can offset the ability of the antiarrhythmics to convert atrial arrhythmias to a regular rhythm.
UNDERSTANDING ANTIARRHYTHMICS
Antiarrhythmics are used to restore normal heart rhythm in patients with arrhythmias. Check this table for information about the indications, adverse reactions, and nursing considerations associated with these drugs.
Life-threatening arrhythmias resistant to other antiarrhythmics
Aggravation of arrhythmias
Hypotension
Anorexia
Severe pulmonary toxicity (amiodarone)
Hepatic dysfunction
Amiodarone increases the risk of digoxin toxicity in patients also taking digoxin.
Monitor blood pressure and heart rate and rhythm for changes.
Monitor for signs of pulmonary toxicity (dyspnea, nonproductive cough, and pleuritic chest pain) in patient taking amiodarone.
CLASS IV ANTIARRHYTHMICS
Diltiazem (Cardizem), verapamil (Calan)
Supraventricular arrhythmias
Peripheral edema
Hypotension
Bradycardia
Atrioventricular block
Flushing (with diltiazem)
Heart failure
Pulmonary edema
Monitor heart rate and rhythm and blood pressure carefully when initiating therapy or increasing dose.
Calcium supplements may reduce effectiveness.
MISCELLANEOUS
Adenosine (Adenocard)
Paroxysmal supraventricular tachycardia
Facial flushing
Shortness of breath
Dyspnea
Chest discomfort
Adenosine must be given over 1 to 2 seconds, followed by a 20 ml flush of normal saline solution.
Record rhythm strip during administration.
Class IB antiarrhythmics
Lidocaine (Xylocaine), a class IB antiarrhythmic, is one of the antiarrhythmics commonly used in treating patients with acute ventricular arrhythmias. Other IB antiarrhythmics include mexiletine (Mexitil).
Class IB drugs work by blocking the rapid influx of sodium ions during the depolarization phase of the heart’s depolarization-repolarization cycle, resulting in a decreased refractory period, which reduces the risk of arrhythmia.
Because class IB antiarrhythmics especially affect the Purkinje fibers (fibers in the heart’s conducting system) and myocardial cells in the ventricles, they’re used only in treating patients with ventricular arrhythmias.
Class IC antiarrhythmics
Class IC antiarrhythmics are used to treat patients with certain severe, refractory (resistant) ventricular arrhythmias. Class IC antiarrhythmics include flecainide (Tambocor), moricizine (Ethmozine), and propafenone (Rythmol).
Class IC antiarrhythmics primarily slow conduction along the heart’s conduction system. Moricizine decreases the fast inward current of sodium ions of the action potential. This depresses the depolarization rate and effective refractory period.
CLASS II ANTIARRHYTHMICS
Class II antiarrhythmics include the beta-adrenergic antagonists, also known as beta-adrenergic receptor blockers. Beta-adrenergic receptor blockers used as antiarrhythmics include:
acebutolol (Sectral)
esmolol (Brevibloc)
propranolol (Inderal).
Class II antiarrhythmics block beta-adrenergic receptor sites in the heart’s conduction system. As a result, the SA node’s ability to fire spontaneously (automaticity) is slowed. The ability of the AV node and other cells to receive and conduct an electrical impulse to nearby cells (conductivity) is also reduced.
Class II antiarrhythmics also reduce the strength of the heart’s contractions. When the heart beats less forcefully, it doesn’t require as much oxygen to do its work.
CLASS III ANTIARRHYTHMICS
Class III antiarrhythmics are used to treat patients with ventricular arrhythmias. Amiodarone (Cordarone) is the most widely used class III antiarrhythmic.
Although the exact mechanism of action isn’t known, class III antiarrhythmics are thought to suppress arrhythmias by converting a unidirectional block to a bidirectional block. They have little or no effect on depolarization.
CLASS IV ANTIARRHYTHMICS
The class IV antiarrhythmics include the calcium channel blockers. These drugs block the movement of calcium during phase 2 of the action potential and slow conduction and the refractory period of calcium-dependent tissues, including the AV node. The calcium channel blockers used to treat patients with arrhythmias are verapamil (Calan) and diltiazem (Cardizem).
ADENOSINE
Adenosine is an injectable antiarrhythmic drug indicated for acute treatment for paroxysmal supraventricular tachycardia. Adenosine depresses the pacemaker activity of the SA node, reducing the heart rate and the AV node’s ability to conduct impulses for the atria to the ventricles.
Antianginals
When the heart’s oxygen demand exceeds the amount of oxygen being supplied, areas of heart muscle become ischemic. When the heart muscle is ischemic, a person experiences chest pain. This condition is known as angina or angina pectoris.
Although angina’s cardinal symptom is chest pain, the drugs used to treat angina aren’t typically analgesics. Instead, antianginal drugs correct angina by reducing myocardial oxygen demand (the amount of oxygen the heart needs to do its work, increasing the supply of oxygen to the heart, or both. (See How antianginals work.)
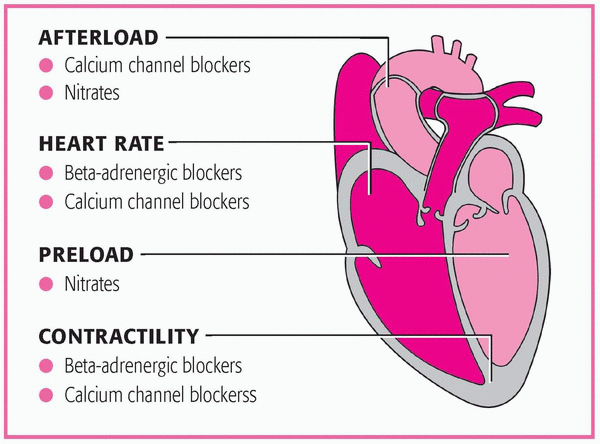
HOW ANTIANGINALS WORK
When the coronary arteries can’t supply enough oxygen to the myocardium, angina occurs. This forces the heart to work harder, increasing heart rate, preload, afterload, and the force of myocardial contractility. Antianginals relieve angina by decreasing one or more of these four factors.
The three classes of commonly used antianginals include:
nitrates (for acute angina)
beta-adrenergic receptor blockers (for long-term prevention of angina)
Nitrates are the drug of choice for relieving acute angina. Nitrates commonly prescribed to correct angina include:
isosorbide dinitrate (Isordil)
isosorbide mononitrate (Imdur)
nitroglycerin (Nitro-Bid).
Nitrates cause the smooth muscle of the veins and, to a lesser extent, the arteries to relax and dilate. This is what happens:
When the veins dilate, less blood returns to the heart.
This, in turn, reduces the amount of blood in the ventricles at the end of diastole, when the ventricles are full. (This blood volume in the ventricles just before contraction is called preload).
By reducing preload, nitrates reduce ventricular size and ventricular wall tension so the left ventricle doesn’t have to stretch as much to pump blood. This, in turn, reduces the heart’s oxygen requirements.
As the coronary arteries dilate, more blood is delivered to the myocardium, improving oxygenation of the ischemic tissue.
UNDERSTANDING ANTIANGINALS
Antianginal drugs are effective in treating patients with angina because they reduce myocardial oxygen demand, increase the supply of oxygen to the heart, or both. Use this table to learn about the indications, adverse reactions, and nursing considerations associated with these drugs.
Long-term prevention of angina (especially Prinzmetal’s angina)
Hypertension
Orthostatic hypotension
Heart failure
Hypotension
Arrhythmias
Dizziness
Headache
Persistent peripheral edema
Pulmonary edema
Monitor cardiac rate and rhythm and blood pressure carefully when initiating therapy or increasing the dose.
Calcium supplementation may decrease the effects of calcium channel blockers.
The arterioles provide the most resistance to the blood pumped by the left ventricle (called peripheral vascular resistance). Nitrates decrease afterload by dilating the arterioles, reducing resistance, easing the heart’s workload, and easing oxygen demand.
BETA-ADRENERGIC RECEPTOR BLOCKERS
Beta-adrenergic receptor blockers are used for long-term prevention of angina, and they’re one of the main types of drugs used to treat hypertension. Beta-adrenergic receptor blockers include:
atenolol (Tenormin)
carvedilol (Coreg)
metoprolol tartrate (Lopressor)
propranolol (Inderal)
Beta-adrenergic receptor blockers decrease blood pressure and block beta-adrenergic receptor sites in the heart muscle and conduction system. Decreasing the heart rate and reducing the force of the heart’s contractions result in a lower demand for oxygen.
CALCIUM CHANNEL BLOCKERS
Calcium channel blockers are commonly used to prevent angina that doesn’t respond to drugs in either of the other antianginal classes. Some calcium channel blockers are also used as antiarrhythmics.
Calcium channel blockers include:
amlodipine (Norvasc)
diltiazem (Cardizem)
nifedipine (Adalat)
verapamil (Calan).
Calcium channel blockers prevent the passage of calcium ions across the myocardial cell membrane and vascular smooth-muscle cells. This causes dilation of the coronary and peripheral arteries, which decreases the force of the heart’s contraction and reduces the heart’s workload.
By preventing arterioles from constriction, calcium channel blockers also reduce afterload. In addition, decreasing afterload decreases the heart’s oxygen demands.
Calcium channel blockers also reduce the heart rate by slowing conduction through the SA and AV nodes. A slower heart rate reduces the heart’s need for oxygen.
Antihypertensives
Antihypertensives, which reduce blood pressure, are used in patients with hypertension, a disorder characterized by high systolic blood pressure, diastolic blood pressure, or both.
Treatment for hypertension begins with beta-adrenergic receptor blockers and diuretics. (See Treating hypertension.) If those drugs aren’t effective, treatment continues with sympatholytic drugs (other than beta-adrenergic receptor blockers), vasodilators, angiotensin-converting enzyme (ACE) inhibitors, angiotensin receptor blockers (ARBs), or a combination of drugs. (See Understanding antihypertensives, pages 152 and 153.)
Sympatholytics
The sympatholytics include several types of drugs but work by inhibiting or blocking the sympathetic nervous system, which causes dilation of the peripheral blood vessels or decreases cardiac output, thereby reducing blood pressure.
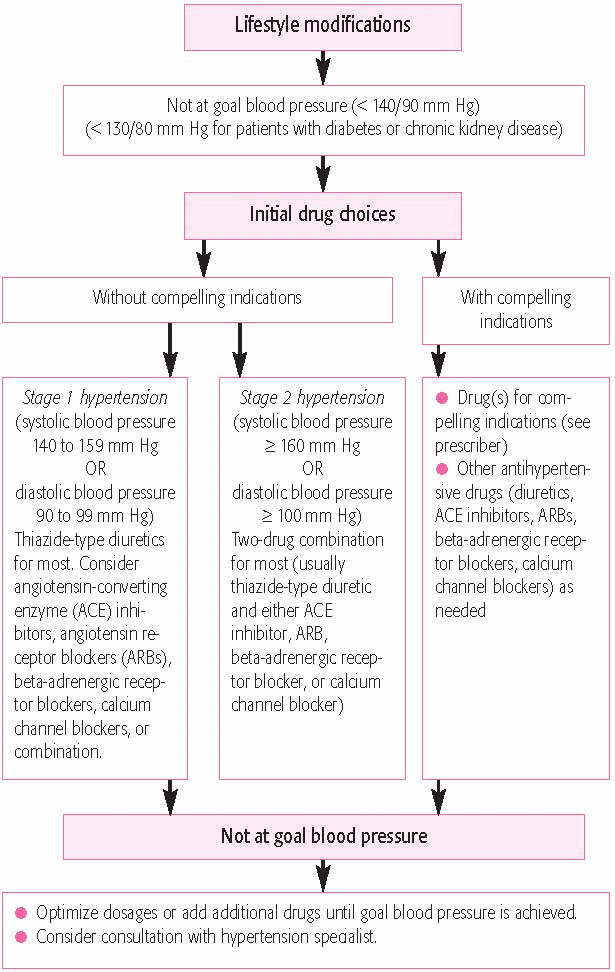
TREATING HYPERTENSION
Below is a flowchart for treating hypertension based on the recommendations of the Joint National Committee on the Detection, Evaluation, and Treatment of High Blood Pressure.
UNDERSTANDING ANTIHYPERTENSIVES
Antihypertensives are prescribed to reduce blood pressure in patients with hypertension. Use this table to learn about the indications, adverse reactions, and nursing considerations associated with these drugs.
DRUGS
INDICATIONS
ADVERSE REACTIONS
NURSING CONSIDERATIONS
SYMPATHOLYTIC DRUGS
Central-acting sympathetic nervous system inhibitors (such as clonidine [Catapres], guanabenz [Wytensin], guanfacine [Tenex], and methyldopa)
Alpha blockers (such as doxazosin [Cardura], phentolamine [Regitine], prazosin [Minipress], and terazosin [Hytrin])
Mixed alpha- and beta-adrenergic receptor blockers (such as labetalol [Normodyne])
Norepinephrine depletors (such as guanadrel [Hylorel])
Hypertension
Hypotension (alpha blockers)
Depression
Drowsiness
Edema
Vertigo (central-acting drugs)
Bradycardia
Hepatic necrosis
Arrhythmias
Monitor blood pressure and pulse before and after administration.
Monitor blood pressure and pulse before and after administration.
The sympatholytic drugs are classified by their site or mechanisms of action and include:
central-acting sympathetic nervous system inhibitors, such as clonidine (Catapres), guanabenz (Wytensin), guanfacine (Tenex), and methyldopa (Aldomet)
alpha blockers, such as doxazosin (Cardura), phentolamine (Regitine), prazosin (Minipress), and terazosin (Hytrin)
mixed alpha- and beta-adrenergic receptor blockers such as labetalol (Normodyne)
norepinephrine depletors such as guanadrel (Hylorel).
Vasodilators
The two types of vasodilators include calcium channel blockers and direct vasodilators. Theses drugs decrease systolic and diastolic blood pressure.
Calcium channel blockers produce arteriolar relaxation by preventing the entry of calcium into the cells. This prevents the contraction of vascular smooth muscle.
Direct vasodilators act on arteries, veins, or both. They work by relaxing peripheral vascular smooth muscles, causing the blood vessels to dilate. This decreases blood pressure by increasing the diameter of the blood vessels, reducing total peripheral resistance.
The direct vasodilators include:
hydralazine (Apresoline)
minoxidil (Loniten)
diazoxide (Hyperstat I.V.)
nitroprusside (Nipride).
Hydralazine and minoxidil are usually used to treat patients with resistant and refractory hypertension. Diazoxide and nitroprusside are reserved for use in hypertensive crisis.
ACE inhibitors
ACE inhibitors reduce blood pressure by interrupting the renin-angiotensin-aldosterone system (RAAS). (See Antihypertensives and the RAAS.)
Commonly prescribed ACE inhibitors include:
benazepril (Lotensin)
captopril (Capoten)
enalapril (Vasotec)
lisinopril (Prinivil)
quinapril (Accupril)
ramipril (Altace).
Here’s how the RAAS works:
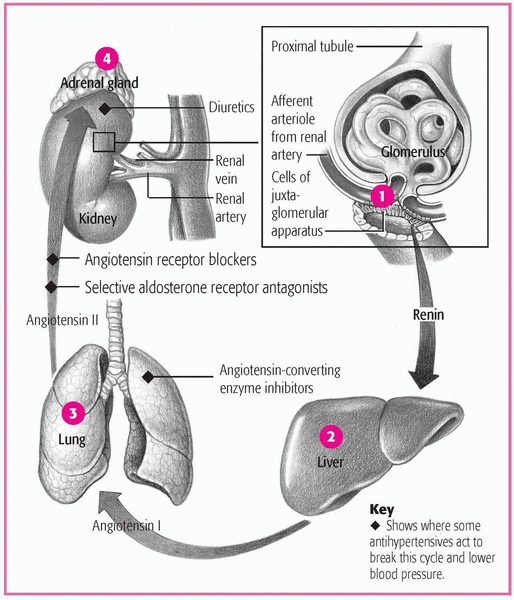
ANTIHYPERTENSIVES AND THE RAAS
The renin-angiotensin-aldosterone system (RAAS) regulates the body’s sodium and water levels and blood pressure.
Juxtaglomerular cells near the glomeruli in each kidney secrete the enzyme renin into the blood.
Renin circulates throughout the body and converts angiotensinogen, made in the liver, to angiotensin I.
In the lungs, angiotensin I is converted by hydrolysis to angiotensin II.
Angiotensin II acts on the adrenal cortex to stimulate production of the hormone aldosterone. Aldosterone acts on the juxtaglomerular cells to increase sodium and water retention and to stimulate or depress further renin secretion, completing the feedback system that automatically readjusts homeostasis.
Normally, the kidneys maintain blood pressure by releasing the hormone renin.
Renin acts on the plasma protein angiotensinogen to form angiotensin I.
Angiotensin I is then converted to angiotensin II.
Angiotensin II, a potent vasoconstrictor, increases peripheral resistance and promotes the excretion of aldosterone.
Aldosterone, in turn, promotes the retention of sodium and water, increasing the volume of blood the heart needs to pump.
ACE inhibitors work by preventing the conversion of angiotensin I to angiotensin II. As angiotensin II is reduced, arterioles dilate, reducing peripheral vascular resistance.
By reducing aldosterone secretion, ACE inhibitors promote the excretion of sodium and water, reducing the amount of blood the heart needs to pump, resulting in a lowered blood pressure.
ANGIOTENSIN II RECEPTOR BLOCKERS
Unlike ACE inhibitors, which prevent production of angiotensin, ARBs inhibit the action of angiotensin II by attaching to tissue-binding receptor sites.
Commonly prescribed ARBs include:
candesartan (Atacand)
irbesartan (Avapro)
losartan (Cozaar)
olmesartan (Benicar)
valsartan (Diovan).
Diuretics
Diuretics are used to promote the excretion of water and electrolytes by the kidneys. By doing so, diuretics play a major role in treating hypertension and other cardiovascular conditions. (See Understanding diuretics.)
The major diuretics used as cardiovascular drugs include:
thiazide and thiazide-like diuretics
loop diuretics
potassium-sparing diuretics.
THIAZIDE AND THIAZIDE-LIKE DIURETICS
Thiazide and thiazide-like diuretics are sulfonamide derivatives. Thiazide diuretics include bendroflumethiazide (Naturetin), hydrochlorothiazide (HydroDIURIL), hydroflumethiazide (Saluron), and methyclothiazide (Enduron). Thiazide-like diuretics include chlorthalidone (Hygroton) and indapamide (Lozol).
UNDERSTANDING DIURETICS
Diuretics are used to treat patients with various cardiovascular conditions. They work by promoting the excretion of water and electrolytes by the kidneys. Use this table to learn about the indications, adverse reactions, and nursing considerations associated with these drugs.
Diuretic-induced hypokalemia in patients with heart failure
Cirrhosis
Nephrotic syndrome
Hypertension
Hyperkalemia
Headache
Nausea
Rash
Monitor electrocardiogram for arrhythmias.
Monitor potassium levels.
Monitor intake and output.
Thiazide and thiazide-like diuretics work by preventing sodium from being reabsorbed in the kidneys. As sodium is excreted, it pulls water along with it. Thiazide and thiazide-like diuretics also increase the excretion of chloride, potassium, and bicarbonate, which can result in electrolyte imbalances.
Initially, these drugs decrease circulating blood volume, leading to a reduced cardiac output. However, if the therapy is maintained, cardiac output stabilizes, but plasma fluid volume decreases.
LOOP DIURETICS
Loop (high-ceiling) diuretics are highly potent drugs. They include:
bumetanide (Bumex)
ethacrynic acid (Edecrin)
furosemide (Lasix).
The loop diuretics are the most potent diuretics available, producing the greatest volume of diuresis (urine production). They also have a high potential for causing severe adverse reactions.
Bumetanide is the shortest-acting diuretic. It’s even 40 times more potent than another loop diuretic, furosemide.
Loop diuretics receive their name because they act primarily on the thick ascending loop of Henle (the part of the nephron responsible for concentrating urine) to increase the secretion of sodium, chloride, and water. These drugs may also inhibit sodium, chloride, and water reabsorption.
POTASSIUM-SPARING DIURETICS
Potassium-sparing diuretics have weaker diuretic and antihypertensive effects than other diuretics, but they have the advantage of conserving potassium.
The potassium-sparing diuretics include:
amiloride (Midamor)
spironolactone (Aldactone)
triamterene (Dyrenium).
The direct action of the potassium-sparing diuretics on the distal tubule of the kidney produces:
increased urinary excretion of sodium and water
increased excretion of chloride and calcium ion
decreased excretion of potassium and hydrogen ion.
These effects lead to reduced blood pressure and increased serum potassium levels.
Spironolactone, one of the main potassium-sparing diuretics, is structurally similar to aldosterone and acts as an aldosterone antagonist.
Aldosterone promotes the retention of sodium and water and loss of potassium; spironolactone counteracts these effects by competing with aldosterone for receptor sites. As a result, sodium, chloride, and water are excreted, and potassium is retained.
Heparin, prepared commercially from animal tissue, is used to prevent clot formation. Low-molecular-weight heparin, such as dalteparin (Fragmin) and enoxaparin (Lovenox), prevents deep vein thrombosis (a blood clot in the deep veins, usually of the legs) in surgical patients.
Because it doesn’t affect the synthesis of clotting factors, heparin can’t dissolve already formed clots. It does prevent the formation of new thrombi, though. Here’s how it works:
Heparin inhibits the formation of thrombin and fibrin by activating antithrombin III.
Antithrombin III then inactivates factors IXa, Xa, XIa, and XIIa in the intrinsic and common pathways. The end result is prevention of a stable fibrin clot.
In low doses, heparin increases the activity of antithrombin III against factor Xa and thrombin and inhibits clot formation. Much larger doses are necessary to inhibit fibrin formation after a clot has formed. This relationship between dose and effect is the rationale for using low-dose heparin to prevent clotting.
Whole blood clotting time, thrombin time, and partial thromboplastin time are prolonged during heparin therapy. However, these times may be only slightly prolonged with low or ultra-low preventive doses.
UNDERSTANDING ANTICOAGULANTS
Anticoagulants reduce the blood’s ability to clot and are included in the treatment plans for many patients with cardiovascular disorders. Use this table to learn about the indications, adverse reactions, and nursing considerations associated with these drugs.
DRUGS
INDICATIONS
ADVERSE REACTIONS
NURSING CONSIDERATIONS
HEPARINS
Heparin and low-molecular-weight heparins, such as dalteparin (Fragmin) and enoxaparin (Lovenox)
Deep vein thrombosis (prevention and treatment)
Embolism prophylaxis
Disseminated intravascular coagulation (heparin)
Prevention of complications after myocardial infarction (MI)
Bleeding
Hemorrhage
Thrombocytopenia
Monitor thromboplastin time; the therapeutic range is 1½ to 2½ times the control.
Monitor the patient for signs of bleeding.
Concomitant administration with nonsteroidal anti-inflammatory drugs, iron dextran, or an antiplatelet drug increases the risk of bleeding.
Protamine sulfate reverses the effects of heparin.
FACTOR XA INHIBITORS
Fondaparinux (Arixtra)
Deep vein thrombosis (prevention and treatment)
acute pulmonary embolism
Hemorrhage
Thrombocytopenia
Nausea
Fever
Not interchangeable with heparin or low-dose heparins.
Monitor the patient for signs of bleeding.
Monitor complete blood count and platelet count.
Monitor anti-Xa levels. Goal for prophylaxis is 0.2 to 0.4 anti-Xa units/ml; goal for therapy is 0.5 anti-Xa units/ml.
ORAL ANTICOAGULANTS
Warfarin (Coumadin)
Deep vein thrombosis prophylaxis
Prevention of complications of prosthetic heart valves or diseased mitral valves
Atrial arrhythmias
Bleeding (may be severe)
Hepatitis
Diarrhea
Monitor prothrombin time and International Normalized Ratio.
Monitor the patient for signs of bleeding.
The effects of oral anticoagulants can be reversed with phytonadione (vitamin K).
Prevention of complications of prosthetic heart valves
Reduction of risk of MI after previous MI or in patients with unstable angina
Prevention of reocclusion in coronary revascularization procedures
GI distress
Bleeding
Thrombocytopenia
Angioedema
Monitor the patient for signs of bleeding.
Aspirin and ticlopidine should be taken with meals to prevent GI irritation.
Dipyridamole should be taken with a full glass of fluid at least 1 hour before meals.
Heparin can be used to prevent clotting when a patient’s blood must circulate outside the body through a machine, such as a cardiopulmonary bypass machine or hemodialysis machine.
FACTOR XA INHIBITORS
Factor Xa inhibitors are a new class of anticoagulants. At this time, the only drug in this class is fondaparinux (Arixtra). Fondaparinux works by inhibiting only factor Xa. Factor Xa is the common point in the intrinsic and extrinsic clotting pathways. Inhibition of factor Xa prevents the formation of thrombin and the formation of a stable fibrin clot.
ORAL ANTICOAGULANTS
Oral anticoagulants alter the liver’s ability to synthesize vitamin K-dependent clotting factors, including prothrombin and factors VII, IX, and X. Clotting factors already in the bloodstream continue to coagulate blood until they become depleted, so anticoagulation doesn’t begin immediately. The major oral anticoagulant used in the United States is warfarin (Coumadin).
ANTIPLATELET DRUGS
Examples of antiplatelet drugs are:
aspirin (Ecotrin)
dipyridamole (Persantine)
ticlopidine (Ticlid)
clopidogrel (Plavix).
Antiplatelet drugs are used to prevent arterial thromboembolism, especially in patients at risk for myocardial infarction (MI), stroke, and arteriosclerosis (hardening of the arteries). They interfere with platelet activity in different drug-specific and dose-related ways.
Low dosages of aspirin (81 mg/day) appear to inhibit clot formation by blocking the synthesis of prostaglandins, which in turn prevents formation of the platelet-aggregating substance thromboxane A2. Dipyridamole and clopidogrel may inhibit platelet aggregation.
Ticlopidine inhibits the binding of fibrinogen to platelets during the first stage of the clotting cascade.
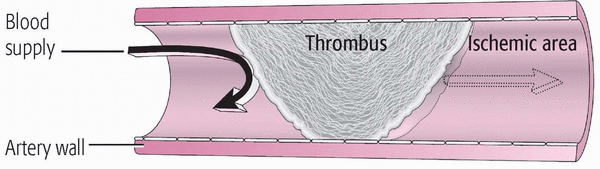
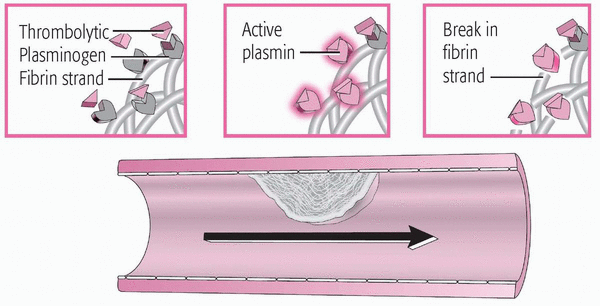
HOW THROMBOLYTICS DISSOLVE CLOTS
When a thrombus forms in an artery, it obstructs the blood supply, causing ischemia and necrosis. Thrombolytics can dissolve thrombi in the coronary and pulmonary arteries, restoring the blood supply to the area beyond the blockage.
Obstructed artery
A thrombus blocks blood flow through the artery, causing distal ischemia.
Inside the thrombus
The thrombolytic enters the thrombus and binds to the fibrin-plasminogen complex, converting inactive plasminogen into active plasmin. Active plasmin digests fibrin, dissolving the thrombus. As the thrombus dissolves, blood flow resumes.
Thrombolytics
Thrombolytics dissolve preexisting clots or thrombi, and they’re commonly used in acute or emergency situations. They work by converting plasminogen to plasmin, which lyses (dissolves) thrombi, fibrinogen, and other plasma proteins. (See How thrombolytics dissolve clots. Also see Understanding thrombolytics, page 164.)
UNDERSTANDING THROMBOLYTICS
Sometimes called clot busters, thrombolytics are prescribed to dissolve a preexisting clot or thrombus. These drugs are typically used in acute or emergency situations. Use this table to learn about the indications, adverse reactions, and nursing considerations associated with these drugs.
Monitor partial thromboplastin time, prothrombin time, International Normalized Ratio, hemoglobin levels, and hematocrit before, during, and after administration.
Monitor vital signs frequently during and immediately after administration. Don’t use an automatic blood pressure cuff to monitor blood pressure.
Monitor puncture sites for bleeding. Don’t use a tourniquet when obtaining blood samples.
Monitor for signs of bleeding.
Some commonly used thrombolytics include:
alteplase (Activase)
reteplase (Retavase)
streptokinase (Streptase).
Adrenergics
Adrenergics are also called sympathomimetics because they produce effects similar to those produced by the sympathetic nervous system.
Adrenergics are classified based on their chemical structure: catecholamines (both naturally occurring and synthetic) and noncatecholamines (See Understanding adrenergics, pages 166 to 169.)
Therapeutic use of adrenergics depends on which receptors they stimulate and to what degree. Adrenergics can affect:
alpha-adrenergic receptors
beta-adrenergic receptors
dopamine receptors.
Most of the adrenergic drugs produce their effects by stimulating alpha- and beta-adrenergic receptors. These drugs mimic the action of norepinephrine or epinephrine.
Dopaminergic drugs act primarily on receptors in the sympathetic nervous system that are stimulated by dopamine.
CATECHOLAMINES
Because of their common basic chemical structure, catecholamines share certain properties. They stimulate the nervous system, constrict peripheral blood vessels, increase heart rate, and dilate the bronchi. They can be manufactured in the body or in a laboratory. Common catecholamines include:
dobutamine (Dobutrex)
dopamine (Intropin)
epinephrine (Adrenalin)
norepinephrine (Levophed)
Catecholamines are primarily direct-acting. When catecholamines combine with alpha or beta receptors, they cause either an excitatory or inhibitory effect. Typically, activation of alpha receptors generates an excitatory response except for intestinal relaxation. Activation of the beta receptors mostly produces an inhibitory response except in the cells of the heart, where norepinephrine produces excitatory effects. (See Learning about adrenergic receptor uses and effects, page 170.)
The effects of catecholamines depend on the dosage and the route of administration. Catecholamines are potent inotropes, meaning they make the heart contract more forcefully. As a result, the ventricles empty more completely with each heartbeat, increasing the heart’s workload and the amount of oxygen it needs to do this harder work.
Catecholamines also produce a positive chronotropic effect, which means they cause the heart to beat faster. That’s because the pacemaker cells in the heart’s SA node depolarize at a faster rate. As catecholamines cause blood vessels to constrict and blood pressure to increase, the heart rate decreases as the body tries to prevent an excessive increase in blood pressure.
Catecholamines can cause the Purkinje fibers to fire spontaneously, possibly producing abnormal heart rhythms, such as premature ventricular contractions and fibrillation. Epinephrine is likelier than norepinephrine to produce this spontaneous firing,
UNDERSTANDING ADRENERGICS
Adrenergic drugs produce effects similar to those produced by the sympathetic nervous system. Adrenergic drugs can affect alpha-adrenergic receptors, beta-adrenergic receptors, or dopamine receptors. However, most of the drugs stimulate the alpha and beta receptors, mimicking the effects of norepinephrine and epinephrine. Dopaminergic drugs act on receptors typically stimulated by dopamine.
Use this table to learn about the indications, adverse reactions, and nursing considerations associated with these drugs.
DRUGS
INDICATIONS
ADVERSE REACTIONS
NURSING CONSIDERATIONS
CATECHOLAMINES
Dobutamine (Dobutrex)
Increase cardiac output in short-term treatment of cardiac decompensation from depressed contractility
Headache, tingling sensation, bronchospasm, palpitations, tachycardia, cardiac arrhythmias (premature ventricular contractions), hypotension, hypertension and hypertensive crisis, angina, nausea, vomiting, tissue necrosis and sloughing (if catecholamine given I.V. leaks into surrounding tissue)
Correct hypovolemia before administering drug.
Incompatible with alkaline solution (sodium bicarbonate); don’t mix or give through same line; don’t mix with other drugs.
Administer continuous drip on infusion pump.
Give drug into a large vein to prevent irritation or extravasation at site.
Monitor cardiac rate and rhythm and blood pressure carefully when initiating therapy or increasing the dose.
Dopamine (Intropin)
Treat shock and correct hemodynamic imbalances
Increase cardiac output
Hypotension
Headache, bradycardia, palpitations, tachycardia, conduction disturbance, cardiac arrhythmias (ventricular), hypotension, hypertension and hypertensive crisis, azotemia, angina, nausea, vomiting, gangrene of extremities in high dose, tissue necrosis and sloughing (if catecholamine given I.V. leaks into surrounding tissue), bronchospasm
Correct hypovolemia before giving drug.
Administer continuous drip on infusion pump.
Give drug into a large vein to prevent extravasation; if extravasation occurs, stop infusion and treat site with phentolamine (Regitine) infiltrate to prevent tissue necrosis.
Monitor cardiac rate and rhythm and blood pressure carefully when initiating therapy or increasing the dose.
Monitor urine output during treatment, especially at high doses.
Give drug into a large vein to prevent irritation or extravasation at site.
Monitor cardiac rate and rhythm and blood pressure carefully when starting therapy or increasing the dose.
CATECHOLAMINES
Norepinephrine (Levophed)
Maintain blood pressure in acute hypotensive states
Anxiety, dizziness, headache, bradycardia, cardiac arrhythmias, hypotension, hypertension, tissue necrosis and sloughing (if catecholamine given I.V. leaks into surrounding tissue), fever, metabolic acidosis, increased blood glucose levels, dyspnea
Correct hypovolemia before giving drug.
Administer continuous drip on infusion pump.
Give drug into a large vein to prevent extravasation; if extravasation occurs, stop infusion, and treat site with phentolamine infiltrate to prevent tissue necrosis.
Monitor cardiac rate and rhythm and blood pressure carefully when starting therapy or increasing the dose.
NONCATECHOLAMINES
Ephedrine
Maintain blood pressure in acute hypotensive states, especially with spinal anesthesia
Treatment of orthostatic hypotension and bronchospasm
Give drug into a large vein to prevent irritation or extravasation at site.
Monitor cardiac rate and rhythm and blood pressure carefully when initiating therapy or increasing the dose.
Phenylephrine (Neo-Synephrine)
Maintain blood pressure in hypotensive states, especially hypotensive emergencies with spinal anesthesia
Restlessness, anxiety, dizziness, headache, palpitations, cardiac arrhythmias, hypertension, tissue necrosis and sloughing (if catecholamine given I.V. leaks into surrounding tissue)
Correct hypovolemia before giving drug.
Administer continuous drip on infusion pump.
Give drug into a large vein to prevent extravasation; if extravasation occurs, stop infusion, and treat site with phentolamine infiltrate to prevent tissue necrosis.
Monitor cardiac rate and rhythm and blood pressure carefully when starting therapy or increasing the dose.
NONCATECHOLAMINES
Noncatecholamine adrenergic drugs have various therapeutic uses because of the many effects these drugs can have on the body such as the local or systemic constriction of blood vessels by phenylephrine (Neo-Synephrine).
Direct-acting noncatecholamines that stimulate alpha activity include methoxamine (Vasoxyl) and phenylephrine.
Those that selectively exert beta2 activity include:
albuterol (Proventil)
isoetharine (Bronkosol)
metaproterenol (Alupent)
Dual-acting noncatecholamines combine both actions and include ephedrine.
These drugs work by blocking impulse transmission (and thus sympathetic nervous system stimulation) at adrenergic neurons or adrenergic receptor sites. The action of the drugs at these sites can be exerted by:
LEARNING ABOUT ADRENERGIC RECEPTOR USES AND EFFECTS
RECEPTOR ACTIVATED
THERAPEUTIC USES
ADVERSE EFFECTS
Alpha1
Control topical superficial bleeding
Treat nasal decongestion
Elevate blood pressure
Delay absorption of local anesthetics
Decrease intraocular pressure
Hypertension
Necrosis with extravasation
Bradycardia
Alpha2
Treat glaucoma
Burning sensation
Ptosis
Redness and swelling of eyelid
Beta1
Treat heart failure, cardiac arrest, and shock
Tachycardia
Arrhythmias
Angina
Beta2
Produce bronchodilation
Delay preterm labor
Hyperglycemia
Tremors
Dopamine
Increase renal blood flow
Increase cardiac output
Elevate blood pressure
Ectopy
Nausea and vomiting
Tachycardia
Palpitations
interrupting the action of sympathomimetics (adrenergics)
reducing available norepinephrine
preventing the action of cholinergics.
Adrenergic-blocking drugs are classified according to their site of action as alpha-adrenergic receptor blockers or beta-adrenergic receptor blockers.
UNDERSTANDING ADRENERGIC BLOCKERS
Adrenergic blockers block impulse transmission at adrenergic receptor sites by interrupting the action of adrenergic drugs, reducing the amount of norepinephrine available, and blocking the action of cholinergics.
Use this table to learn the indications, adverse reactions, and nursing considerations needed to safely administer these drugs.
Beta-adrenergic receptor blockers can alter the requirements for insulin and oral antidiabetics.
ALPHA-ADRENERGIC RECEPTOR BLOCKERS
Alpha-adrenergic receptor blockers work by interrupting the actions of sympathomimetic drugs at alpha-adrenergic receptors. This results in:
relaxation of the smooth muscle in the blood vessels
increased dilation of blood vessels
decreased blood pressure.
Drugs in this class include phentolamine and prazosin.
Ergotamine (Ergomar) is a mixed alpha agonist and antagonist. At high dose, it acts as an alpha-adrenergic receptor blocker.
Alpha-adrenergic receptor blockers work in one of two ways:
They interfere with or block the synthesis, storage, release, and reuptake of norepinephrine by neurons.
They antagonize epinephrine, norepinephrine, or adrenergic (sympathomimetic) drugs at alpha-receptor sites.
Alpha-receptor sites are either alpha1 or alpha2 receptors. Alpha-adrenergic receptor blockers include drugs that block stimulation of alpha1 receptors and that may block alpha2 stimulation.
Alpha-adrenergic receptor blockers occupy alpha-receptor sites on the smooth muscle of blood vessels.
This prevents catecholamines from occupying and stimulating the receptor sites. As a result, blood vessels dilate, increasing local blood flow to the skin and other organs. The decreased peripheral vascular resistance helps to decrease blood pressure.
BETA-ADRENERGIC RECEPTOR BLOCKERS
Beta-adrenergic receptor blockers, the most widely used adrenergic blockers, prevent stimulation of the sympathetic nervous system by inhibiting the action of catecholamines and other sympathomimetic drugs at beta-adrenergic receptors.
Beta-adrenergic drugs are selective or nonselective. Nonselective beta-adrenergic drugs affect:
beta1-receptor sites (located mainly in the heart)
beta2-receptor sites (located in the bronchi, blood vessels, and the uterus).
Nonselective beta-adrenergic drugs include carvedilol, labetalol, propranolol, sotalol (Betapace), and timolol (Blocadren).
Selective beta-adrenergic receptor blockers primarily affect the beta1-adrenergic sites. They include acebutolol, atenolol, esmolol and metoprolol.
Some beta-adrenergic receptor blockers such as acebutolol have intrinsic sympathetic activity. This means that instead of attaching to beta receptors and blocking them, these beta-adrenergic receptor blockers attach to beta receptors and stimulate them. These drugs are sometimes classified as partial agonists.
Beta-adrenergic receptor blockers have widespread effects in the body because they produce their blocking action not only at the adrenergic nerve endings but also in the adrenal medulla. Effects on the heart include:
Only gold members can continue reading. Log In or Register to continue