Chapter 42 Treatment of the Stable Patient with Chronic Obstructive Pulmonary Disease
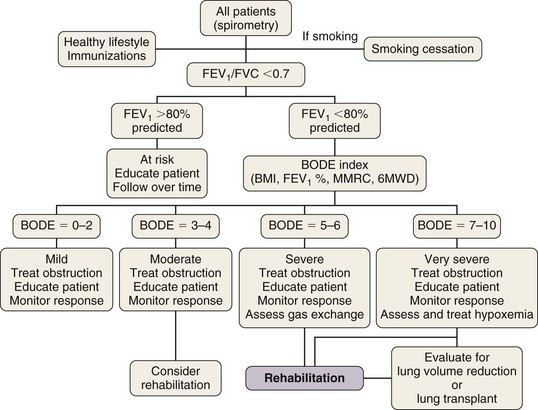
Box 42-1 summarizes the available therapeutic options for patients with COPD. This chapter reviews medical management of COPD that centers on three goals: (1) prevent deterioration in lung function, (2) alleviate symptoms, and (3) treat complications as they arise. Once diagnosed, patients with COPD should be encouraged to participate actively in their management; collaborative management improves their self-reliance and self-esteem. All patients should be encouraged to lead a healthy life and exercise regularly. Preventive care is extremely important, and all patients should receive immunizations, including pneumococcal vaccine every 5 years and yearly influenza vaccine. Figure 42-1 provides an algorithm detailing this comprehensive approach.
Box 42-1
Therapy of Patients with Symptomatic Stable Chronic Obstructive Pulmonary Disease
Multicomponent Disease
Based on the multidimensional nature of COPD and the availability of multiple effective therapies, the approach shown in Figure 42-1 may more accurately help clinicians evaluate patients and choose therapies than the current approach, using primarily the FEV1 percentage from reference values.
Respiratory Manifestations
Pharmacologic Therapy of Airflow Obstruction
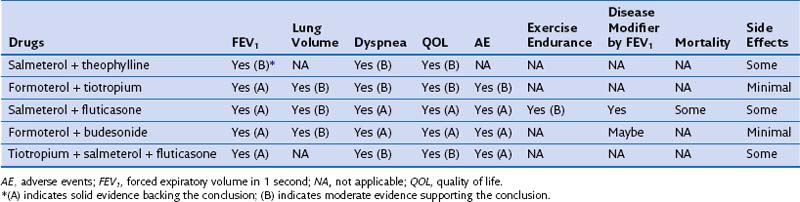
Most patients with COPD require pharmacologic therapy. This should be organized according to the severity of symptoms, the degree of lung dysfunction, and the tolerance of the patient to specific drugs. A stepwise approach similar to that developed for systemic hypertension may be helpful, because medications alleviate symptoms, improve exercise tolerance and QOL, and may decrease mortality. Tables 42-1 and 42-2 summarize the evidence supporting the effect of individual and combined therapies on outcomes of importance in patients with COPD. Because most patients with COPD are elderly, care must be taken when prescribing drugs for this population. Comorbidities are frequently present in patients with COPD, mandating caution to ensure that therapy takes these into account.
Table 42-1 Effect of Single Pharmacologic Agents on Important Outcomes in Chronic Obstructive Pulmonary Disease Patients
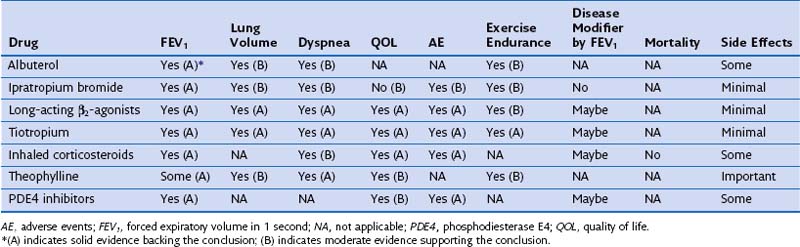
Table 42-2 Effect of Combined Pharmacologic Agents on Important Outcomes in Chronic Obstructive Pulmonary Disease Patients