How to Use the Flip and See
 How to Use the Flip and See Portion of This Book
How to Use the Flip and See Portion of This Book
Please turn to the Rhythms section of this book for the next exercise. To use the Flip and See Rhythms section:
1 Separate the pages at the perforated line.
2 Flip just the right side of the book to create variations of rhythms.
3 Compare the rhythms side by side to see how the abnormal tracing looks next to the normal one.
To use this section as a reference text, you can view the rhythms in full strips across the page.
In reading three-lead and 12-lead electrocardiograms (ECGs), practitioners ask themselves, “How does this compare to the normal sinus rhythm?”
 Flip and See Guided Tutorial
Flip and See Guided Tutorial
Here is a brief explanation of the defining characteristics of each rhythm. Try to view each rhythm as a pattern.
1 With both sides of normal sinus rhythm (p. 137) placed side by side, take a look at the pattern. All the intervals are regular and normal, with no bizarre ectopic activity. The rate is 80 beats per minute; the R-R intervals are regular. Count a 6-second strip.
4 Flip just the right side, to p. 143. This one looks normal but fast: 140 beats per minute. Anything over 100 beats per minute is considered sinus tachycardia. (The prefix tachy– means fast.) This can be a response to certain conditions, such as fever, fright, or hypoxia. When the rate starts to go very fast, P waves can be buried in the preceding complex.
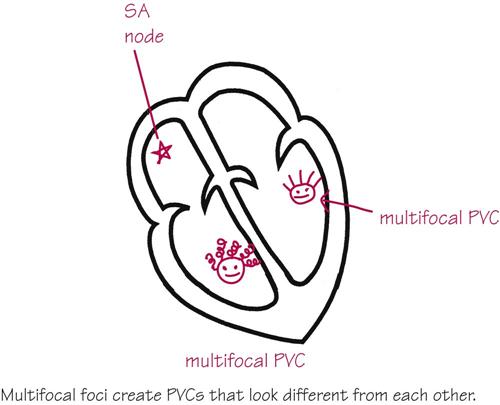
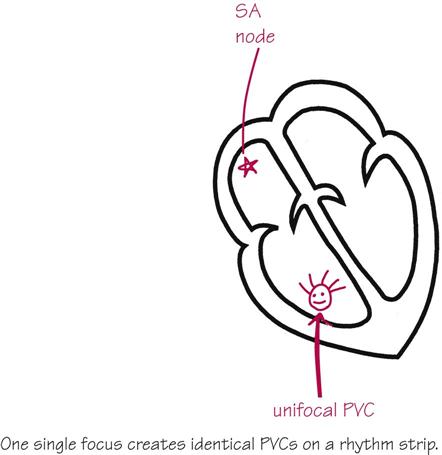
6 Flipping to p. 147, the first complex on the right-hand side of the page is certainly wide and definitely bizarre looking. This is called a premature ventricular contraction. If all of the wide, bizarre complexes look the same, they are called unifocal premature ventricular contractions, because they come from the same place in the ventricles. If they look wide, bizarre, and different, they are called multifocal premature ventricular contractions. The strip on p. 147 illustrates multifocal premature ventricular contractions.
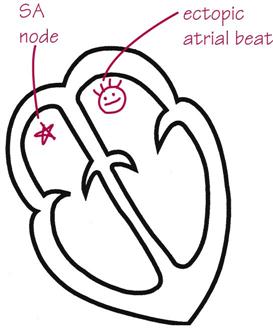
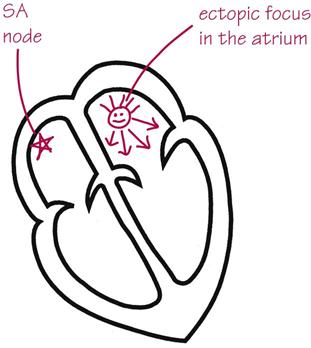
7 Flip to p. 149. Are there any P waves present, or are those all P waves? Actually, they are all flutter waves, also known as F waves. In atrial flutter, an ectopic focus in the atrium is beating fast, up to 350 beats a minute. In this illustration the atria are beating at 210 times a minute. The AV node is acting as a gatekeeper and allowing only every third impulse to contract the ventricles.
8 Flip just the right side of p. 151. This rhythm shows many weak ectopic foci in the atria. This produces an uncoordinated beating of the atria and a “bag of worms” effect. In atrial fibrillation, the baseline may appear to have a few actual P waves, but it is made up mostly of f waves. The lower case f stands for fibrillatory. The R-R interval is irregular in this rhythm, because eventually all these small atrial contractions generate an impulse large enough to conduct to the ventricles.
 Excuse me…
Excuse me…
How can you tell the difference between atrial fibrillation and normal sinus rhythm in a bouncy ambulance when the baseline is wavy? Answer…
Answer…
Check the R-R interval. Normal sinus rhythm has regular R-R intervals, whereas atrial fibrillation has irregular R-R intervals. In normal sinus rhythm with a bouncy baseline or a loose lead, the R-R interval remains constant, whereas in atrial fibrillation, the many weak foci in the atria make the R-R interval irregular in appearance and measurement. Place p. 137 (normal sinus rhythm with loose leads) and p. 151 (atrial fibrillation) together and look at the difference.
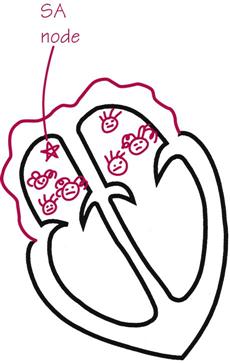
9 Return the booklet to normal sinus rhythm on the left. Turn just the right side of the page to resume the lesson, on p. 153. Supraventricular tachycardia or paroxysmal supraventricular tachycardia is a fast heart rate, 140-250 beats per minute. Supraventricular tachycardia originates above (supra-) the ventricles but below the sinoatrial (SA) node. It is characterized by a rapid heart rate, one that is so fast that sometimes the P wave is buried in the preceding complex. Excuse me…
Excuse me…
How can I distinguish a fast sinus tachycardia from a supraventricular tachycardia? Answer…
Answer…
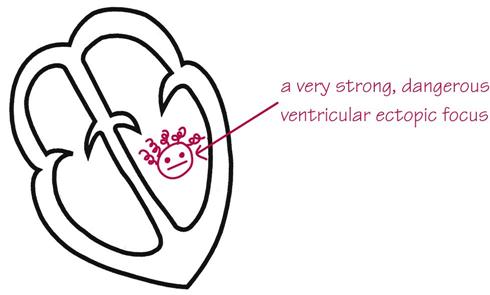
10 Flip just the right side of p. 155. This rhythm is extremely dangerous: ventricular tachycardia. This is an ectopic focus in the ventricles gone wild. Immediate intervention is needed here. The patient may be stable and talking, unstable, or even pulseless.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


