Fig. 2.1
Thoracoscopy in 1912: Jacobaeus
1913 is also remembered in the field of thoracoscopy because in that year at the hospital of St. Göran in Stockholm, Jacobaeus sectioned “with the thoracoscope as a guide, fragments of pulmonary pleura in a case of pleural tumour”, thereby making the first attempt to perform lysis of pleural adhesions, and continued “with an even smaller trocar, I introduced an instrument similar to larynx scissors, and cut a small piece from the pulmonary area. There was no discomfort for the patient either during or after the operation”. On 21 May 1914, he performed a thoracoscopy under local anaesthesia for the management of a case of cavitary pulmonary tuberculosis. This procedure used separate entry portals for the optic and the cautery, in the fifth and third intercostal space, respectively. He saw a false adherence which joined the parenchyma to the diaphragm and a true one located on the right upper lobe, the size of a little finger. He cauterised it, causing the instant collapse of the lung. The patient returned to his room on foot, and there were no immediate consequences. On 23 May a new insufflation of air was carried out: 300 cc with a pressure of +7 cm H2O; this was considerably lower than that used prior to the intervention. The outcome was positive, with the cessation of expectoration within a few days. An examination a month later showed that the lung remained collapsed, the cavity was compressed, and the patient was well.
In subsequent years (Fig. 2.2) his described clinical techniques including thoracoscopic lysis of adhesions which were preventing pneumothorax (later to be known as the “Jacobaeus operation”) became more numerous. They were published in international journals such as the British Medical Journal and the American Review of Tuberculosis, where the first 78 cases treated with 55 positive results were reported.

Fig. 2.2
Thoracoscopy in 1920: Jacobaeus
Two other articles go into more detail: one in English which was published in 1923 in the Archives of Radiology and Electrotherapy, from the Proceedings of the Royal Society of Medicine, and a more extensive review published in German entitled “Die Thorakoskopie und ihre praktische Bedeutung” (Thoracoscopy and its practical meaning) (Jacobaeus 1925). This comprehensive paper details all of Jacobaeus’ clinical work and includes five drawings of the main endoscopic features encountered, of which three of the images were primarily concerned with tuberculosis pleural effusions. The paper also included a photograph which demonstrated the exact position of the hands and the correct positioning of the trocar during the operation. More attention is paid to tuberculosis than to tumours, which comprises 30–40 cases; these are endoscopically distinguishable from tuberculosis by being characterised by lesions with nodules-masses and/or pleural thickening. In the cases with tumours, there is a clear prevalence of metastatic pleurisy, but Jacobaeus also described five cases with the non-specific term “endothelioma”. In his conclusions he stresses that thoracoscopy, preceded by careful examination of x-rays and preparatory pneumothorax, is fundamental in order to achieve accurate diagnosis of the nature and cause of any type of pleural tumour.
Jacobaeus also worked closely with the thoracic surgeon at his hospital, Einar Key, which enabled an appropriate and complete management of intrathoracic pathologies. In 1922 an article was published in Surgery, Gynecology and Obstetrics entitled “The practical importance of thoracoscopy in surgery of the chest” which gives an account of five cases of thoracoscopy prior to therapeutic thoracotomy. In these cases Jacobaeus first induces a pneumothorax and examines the pleural cavity, identifying the endothoracic tumour and providing useful information for the subsequent thoracotomy.
Jacobaeus was willing to collaborate with anyone who was interested in the field of research he had created and was in turn respected and recognised without envy as the initiator of thoracoscopy. For example, together with Unverricht, he improved the technical characteristics of the thoracoscope to make it more reliable and effective and always cited the contribution of others in his work.
2.4 Diffusion of the Method
The path opened by Jacobaeus was rapidly followed by others, and the application of the method spread to various countries.
In France, notable physicians were Dumarest, author of an important paper on artificial pneumothorax (Dumarest et al. 1954), and Douady and Meyer, whose manual on pleuroscopy and sectioning of adhesions was widely circulated (Douady and Meyer 1942).
In Germany the initiator of thoracoscopy was Unverricht, who introduced it in 1915 and collaborated with Jacobaeus in the creation of the instrument that was most commonly used at that time. His personal experience comprised of approximately 2,500 interventions (Fig. 2.3), and he published a short article on the method (Unverricht 1923) which was illustrated with explanatory watercolours. Other important German physicians in this field included Diehl and Kremer who published a complete monograph on the subject (Diehl and Kremer 1929).
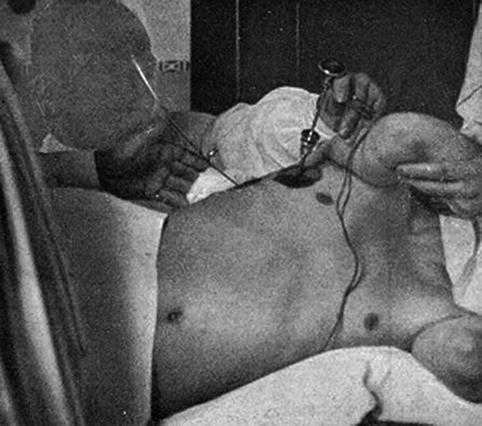
Fig. 2.3
Thoracoscopy in 1925: Unverricht
In 1923 in Scandinavia, Holmböe designed special haemostatic forceps with a mechanical action to prevent haemorrhage, and Güllbring worked extensively on improving the illumination of the optic and also invented an adjustable operating bed which was widely used in Europe. He extended the treatment of lysis of adhesions even in cases with apparent complete pneumothorax.
Singer and Davidson became known in the United States mainly for the introduction of complex combined instruments in the attempt to replace the old thoracoscope, which, despite their efforts, remained the instrument of preference (Fig. 2.4). However, the most significant American contribution came from Matson (Fig. 2.5), who performed 350 interventions over a 15-year period and adopted an effective strategy to avoid endopleural haemorrhage, using the recently introduced electrocautery scalpel with excellent results (Matson 1936).
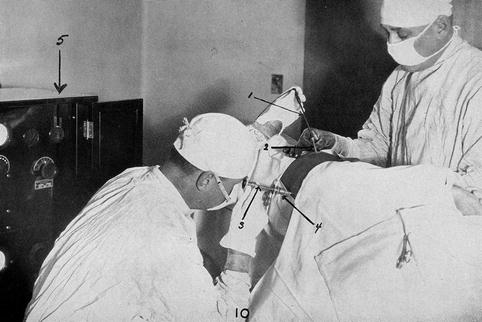

Fig. 2.4
Thoracoscopy in 1929: Matson
Fig. 2.5
Thoracoscopy in 1926: unknown
In Switzerland the most important contribution came from G Maurer, a thoracic surgeon in Davos, who, concerned by the problem of frequent haemorrhage, developed a technique to isolate the point of attachment of adhesions.
Chandler was undoubtedly the best-known thoracoscopist in Britain of that period, and he is noted for the introduction of his eponymous combined thoracoscope. This instrument had an optical deviation of 30° which permitted the rapid passage from coagulation to sectioning of the adhesions without changing cautery. It was used principally in Britain and was described in a 1930 article in the Lancet, which was an important contribution regarding thoracoscopy in a journal with such a wide distribution (Chandler 1930).
In Spain in 1924, Xalabarder invented a simple new technique of transillumination of adhesions by placing the cautery behind them and bringing it quickly to a high temperature, thereby generating an intense red-white light. The Portuguese Lopo de Carvalho, a noted scholar of pulmonary angiography, was among the first to use thoracoscopy in the treatment of tuberculosis.
The Canadian thoracic surgeon Norman Bethune (1890–1939) designed a number of new instruments which were integrated with existing ones. He patented lights to transilluminate adhesions and invented staples to position adherences before sectioning, and his name is connected to the first nebulisation of talc in the pleural cavity (Bethune 1935).
In Italy, Stolkind was the first to use the thoracoscope; and in 1914 he wrote, referring to the experience of Jacobaeus, that “ la toracoscopia rappresenta uno degli importanti mezzi ausiliari di diagnosi dei tumori del cavo pleurico, dei noduli tubercolari e del punto di lacerazione del polmone nel pneumotorace” (thoracoscopy represents one of the important auxiliary methods of diagnosis of tumours of the pleural cavity, of tubercular nodules and the point of laceration of the lung in pneumothorax) (Stolkind 1914). But the brightest star was Felice Cova, who was called the “Paganini of the thoracoscope” because of his consummate skill and dexterity with the instrument and who published a magnificent book entitled the Atlas Thoracoscopicon which includes many excellent didactic illustrations (Cova 1928).
A large number of books on the subject of thoracoscopy were published in that period – in various countries and languages. These were copiously illustrated and by and large complete works. Some of the most significant texts are those by Unverricht (Unverricht 1923), Cova (Cova 1927), and Dihel and Kramer (Diehl and Kremer 1929). But perhaps the most complete is that by Mistal, a Swiss physician entitled “Endoscopie et pleurolyse” with a preface by Jacobaeus. It is a comprehensive monograph of 400 pages in 11 chapters with numerous drawings and photographs including 557 bibliographical references (Mistal 1935).
There is no doubt that thoracoscopy was the principal method used for the lysis of adhesions (Fig. 2.6) (Jacobaeus operation) as it now had become reliable and recognised both experimentally and in practice. Dedicated endoscopic rooms were developed, nursing staff were appropriately trained, and thorax models were created and widely distributed in order to teach the Jacobaeus operation.
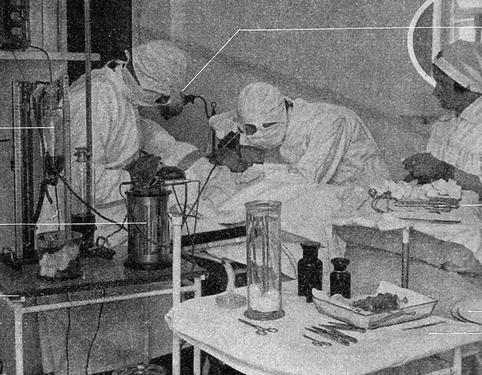
Fig. 2.6
Thoracoscopy in the 1930s: unknown
However, there was no improvement to biopsy forceps (staging of endothoracic cancer was still being carried out with open thorax). There was still no talk of pleurodesis, pneumothorax prior to the examination of the pleural cavity was seen as a dangerous manoeuvre, and even biopsy was considered unsafe because of the risk of haemorrhage.
But diagnostic thoracoscopy, for indications other than tuberculosis and without performing therapeutic pneumothorax, had begun.
At first only anecdotal evidence suggested the verification of occasional cases of metastatic tumours or mesothelioma or cases of spontaneous pneumothorax. For example, the French physicians Sergent and Kourilsky published in the “Travaux originaux” section of Presse Medicale an article entitled “Contribution a l’ étude de l’endothéliome pleural – Image radiologique e pleuroscopique” (Contribution to the study of pleural endothelioma – radiological and pleuroscopic image). It discusses the case of a 62-year-old patient with a history of repeated thoracentesis, parietal thoracic swelling, and radiological verification of pleural nodules. Pleuroscopy was carried out for diagnosis with only a macroscopic exam performed and without tissue biopsy (Sergent and Kourilsky 1939). This initial contribution was followed by a paper from Fourestier and Duret who maintained, again in the Presse Medicale that pleural biopsy is essential for the diagnosis of endothelioma, citing three clinical cases they had observed (Fourestier and Duret 1943). They stressed the importance of distinguishing between true primary pleural tumours (endotheliomas), which are extremely rare, and pulmonary tumours which develop later and are more common. In reality the two pathologies, although prognostically very different, “sont parfaitement susceptibles de revêtir la même morphologie” (are perfectly capable of assuming the same morphology).
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


