The Tobacco Epidemic
Carolyn Dresler
Tobacco has a fascinating history. Tobacco is native only to the Americas and its scientific names include Nicotiana rustica and Nicotiana tabacum.1 Tobacco was first experienced by Europeans when Columbus discovered the Americas in 1492 when they saw natives smoking “a kind of plant” while exploring what is now Cuba. The first two Europeans to see this smoking, Rodrigo de Jerez and interpreter Luis de Torres, even tried it themselves, becoming the first Europeans to experience tobacco.1 Tobacco was brought back to the European countries where it rapidly spread in usage. Reportedly within 3 months after Columbus returned to Spain, the two Europeans to first experience tobacco were perpetual users of the plant. Quite quickly, the addictive nature of tobacco was noted by the Spanish, which was a novel experience for Europeans—this habitual use was felt to be un-Christian, and therefore declared a “sin.”1
However, there was no turning back. Tobacco rapidly became a cash crop, with the product flowing from the New World to support the growing number of users in the Old World. Jamestown, much to the dismay of King James, was able to become solvent as a result of tobacco production from 1610 to 1620.2 When King James could no longer prevent Jamestown from shipping tobacco, he placed the first New World tax—on tobacco!2 In many places in the new colonies, tobacco was used as a form of currency.2 Tobacco cultivation spread throughout many of the colonies, and with the patent of the new Bonsack machine in 1881, which more efficiently mechanized production, the manufacturing of cigarettes began.2 With the increasing widespread marketing of cigarettes, the death toll also began to increase.
Globally, in high-income countries, tobacco is the major causative agent for three of the top five causes of death for 2005: heart disease, stroke, lung cancer, lower respiratory infections, and chronic obstructive pulmonary disease (COPD).3 It is predicted that by 2030, 8.3 million people globally will die from tobacco-induced disease, and tobacco will be responsible for 10% of all deaths globally.4 Smokers will lose on average 10 years of life and 50% of people who smoke will die of a tobacco-related disease.5 At present, globally there are a total of 848,132 lung cancer deaths in men (age-standardized rate [ASR]: 31.2) and 330,786 deaths in women (ASR: 10.3).6 Overall, lung cancer is the number one cause of cancer deaths, accounting for 17.6% of the total number of deaths. Lung cancer is the leading cause of cancer death in men worldwide; however, the picture is a little more complicated with either breast or lung cancer being the number one cause of cancer deaths in women. The relationship of breast to lung cancer deaths often reflects the prevalence of smoking among women. Figure 2.1 illustrates the age-standardized incidence of lung cancer for regions around the world, which reflects the regions’ historical use of tobacco.6
The tobacco epidemic is rapidly changing around the world, and it varies from country to country, mostly according to the state of economic development. Figure 2.2 illustrates the Lopez curve of the tobacco epidemic.7 This model was developed from the 100-plus year history of smoking, particularly in the developed world. As demonstrated in Figure 2.2, a few decades after the peak in smoking prevalence, a country experiences a peak in lung cancer deaths. This model is even more powerful when gender is considered. When comparing gender-related prevalence and rate of deaths, the tobacco epidemic may then be divided into four stages. Stage I is one of quite low male and female prevalence of smoking and few smoking-related deaths. Many low-income countries, such as in sub-Saharan Africa, are in this stage. Stage II consists of a rapid rise in the number of male smokers to its peak, a start in the rise in female smokers, an upswing in the number of male deaths, but still few deaths in women. In stage III, the prevalence of male smoking begins to decline, female smoking is still increasing, and the rate of smoking-attributed male deaths is at its peak (around 30% of all deaths) with the rates for women beginning to sharply increase. In stage IV, female smoking peaks and then declines as male smoking continues
to decline and smoking-attributable death for men and women decreases. Countries such as the United States and United Kingdom would be characteristic of stage IV, where the rates of female smoking-attributable deaths are just reaching their peaks, while the males rates have already started their decline.
to decline and smoking-attributable death for men and women decreases. Countries such as the United States and United Kingdom would be characteristic of stage IV, where the rates of female smoking-attributable deaths are just reaching their peaks, while the males rates have already started their decline.
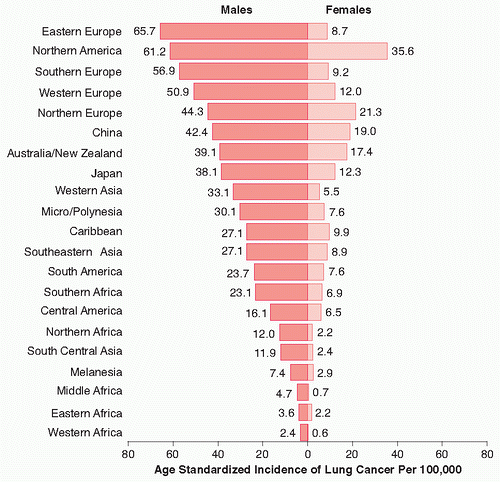 FIGURE 2.1 Age-standardized incidence of lung cancer for regions around the world. Data shown per 100,000 by sex. (From Parkin DM, Bray F, Ferlay J, et al. Global cancer statistics, 2002. CA Cancer J Clin 2005;55:74-108.) |
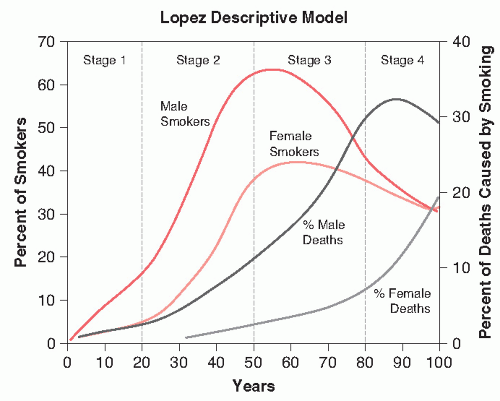 FIGURE 2.2 Stages of the tobacco epidemic—the Lopez Descriptive Model. (From Lopez AD, Collishaw NE, Piha T. A descriptive model of the cigarette epidemic in developed countries. Tob Control 1994;3:242-247.) |
In the United States, cigarettes are by far the predominant form of tobacco consumption, as seen in Figure 2.3.8 This pattern is seen around the world as the tobacco industry increasingly focuses outside of the more developed economies and into the more developing economies. The leading tobacco leaf importers are the Russian Federation, United States, Germany, Netherlands, Japan, United Kingdom, France, Belgium, Ukraine, and China. However, the top tobacco leaf exporters are very different: Brazil, China, United States, Zimbabwe, Italy, India, Turkey, Malawi, Greece, Argentina.9 (China, Brazil, India, and the United States produce over two thirds of the 2004 global tobacco crop. India uses a significant proportion of their tobacco for smokeless use.)9 Thus, the developing countries are more likely to grow and export the tobacco to the richer countries who then manufacture the finished cigarettes. In fact, Altria (the new name for Philip Morris) is the largest transnational tobacco manufacturer, and it is located in the United States. Philip Morris also has the number one global brand of cigarettes: Marlboro, and they sell them in 160 countries of the world.9 The second largest company is British American Tobacco, located in the United Kingdom, and they have one seventh of the global market. Number three is Japan Tobacco and number four is Imperial Tobacco located in United Kingdom, and these four companies comprise 43% of the market. The largest tobacco manufacturer is the China National Tobacco Corporation, which controls 34% of the market—most of which is still within China. This, of course,
speaks to the size of the Chinese population and the approximately 60% of men who smoke.9
speaks to the size of the Chinese population and the approximately 60% of men who smoke.9
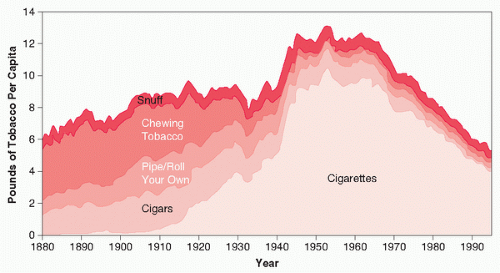 FIGURE 2.3 Per capita consumption of different forms of tobacco in the United States, 1880 to 1995. (From Burns DM, Lee L, Zhen LA, et al. Cigarette smoking behavior in the United States. In: Burns D, Garfinkel L, Samet J, eds. Changes in Cigarette-Related Disease Risks and Their Implication for Prevention and Control; Monograph 8. Bethesda, MD: National Institutes of Health, 1997:13.) |
Global cigarette consumption has grown dramatically over the past few decades. The global cigarette consumption has gone from 10 billion sticks to 2150 billion sticks in 1960, to 5604 billion sticks in 2002, with an estimated 9 trillion cigarettes in 2025. The top five consumers of cigarettes are China, United States, Russian Federation, Japan and Indonesia.9
It is no wonder that the trends for tobacco-related deaths have steadily climbed as cigarette consumption increases. For example, the smoking-related mortality in men in the United Kingdom went from 27% in 1955 to 34% in 1985 and dropped to 27% in 1995, whereas in former socialist countries, the smoking-related mortality in men went from 1.3% in 1955 to 3.7% in 1985 to 5.2% in 1995. 10 This may seem like a low number in former socialist countries; however, in 2001, the smoking prevalence in Belarusian men was 56%, Georgian men 53%, Kazakhstan men 65%, and Russian men 60%.11 The smoking prevalence rates in women, as of 2001, were relatively low (<10%); however, the tobacco industry is undoubtably targeting this potentially growing market. Evidence has already demonstrated the significant increases in cigarette production in parallel with increased consumption in the countries of the former Soviet Union who have had outside investments from the transnational tobacco industries.12 There is enough experience to predict the tremendous death toll that these smoking prevalences will have in future years. In China, two thirds of men start smoking before the age of 25, and with projections, 100 million of the current 300 million Chinese men younger than the age of 30 will be killed by tobacco.10
Figure 2.4 demonstrates the comparison of cigarette consumption between the United States and Japan from 1990 to the present.5 With these curves in mind, Figures 2.5 and 2.65 demonstrate the trends in lung cancer mortality in six different countries, including the United States and Japan—all are considered industrialized, “western” economies. It is striking to observe the differences between even these “westernized” economies and between the sexes. It is clear that the United Kingdom, followed by the United States had the earliest and most dramatic decline in male lung cancer death rates, whereas the picture for the women—as predicted by the Lopez curves, lags significantly behind.
It is also very important to consider the state of tobacco control within each country and how this impacts the smoking prevalence rates. Western countries have been at the forefront of tobacco control, with the resultant decrease in the number of people starting smoking, but also importantly, the number of people quitting smoking. Figures 2.7 and 2.8 demonstrate the age-specific prevalence of current and former smokers by birth cohort in U.S. men and Japanese men.5 It is striking to observe the differences in age of onset of smoking and the numbers of former smokers (those who have quit). These differences explain the differences in the lung cancer mortality age-specific curves in Figure 2.5.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


