(1)
Department of General surgery, Fuwai Hospital, Beijing, China
3.1 General Considerations
3.1.1 Location
The right atrium (RA) is the right upper chamber of the heart and is located above the RV (Fig. 3.1). After the pericardium is opened, the lateral free wall can be seen directly (Fig. 3.2). The free wall is the common area for cannulation and surgical approaches into the heart. The vena cava orifices, aortic sinus, and LA are located around the RA (Fig. 3.3). The anterior wall of the RA is located very close to the right coronary cusp (Fig. 3.4). The atrioventricular node is in front of the septal leaflet of the TV, in the posteroinferior portion of the membranous ventricular septum (Fig. 3.5). The interatrial groove is located between the right and left atria (Fig. 3.6).
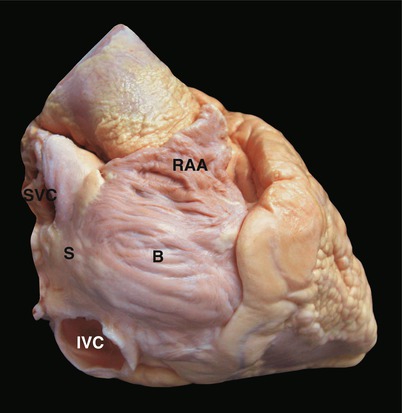
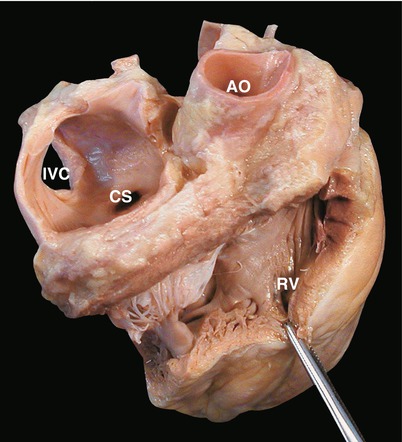
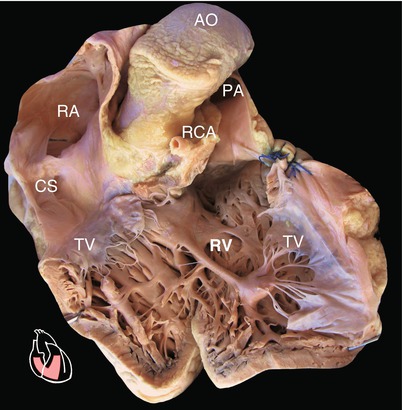
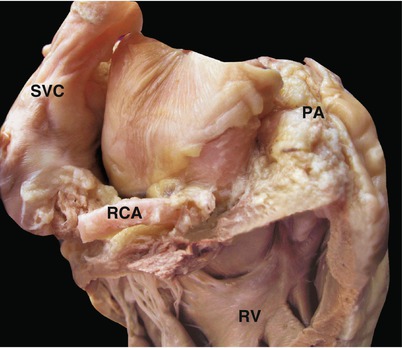
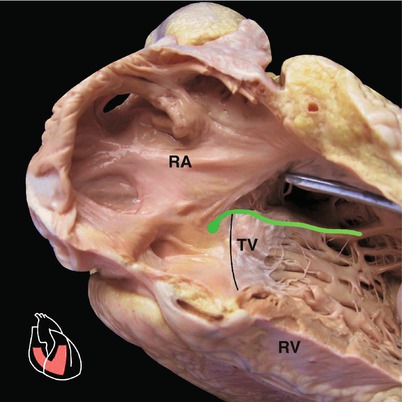
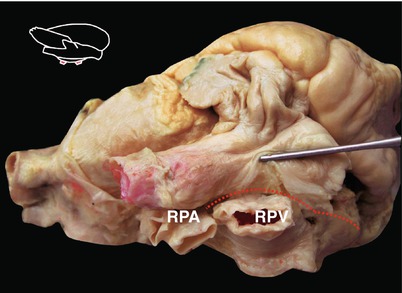
Fig. 3.1
Appearance of the right atrium (RA). The RA is located above the RV and behind and to the right of the root of the aorta. The main structure of the RA, including the sinus venosus and body of the RA, can be seen perfectly from the right lateral side. Usually, the lateral free wall of the body portion is chosen to make the incision. B body of RA, IVC inferior vena cava, RAA right atrium appendage, S sinus venosus portion of RA, SVC superior vena cava
Fig. 3.2
Location of the right atrium in the heart (anatomy position). After the outer free wall of the RA is incised, the sinus venosus portion, including the coronary sinus, the IVC, and the posterior wall of the RA, is shown well. AO aorta, CS coronary sinus, IVC inferior vena cava, RV right ventricle
Fig. 3.3
Frontal plane of the heart (anatomy position). The elementary structures and connection, transition of RA, and RV are revealed. PA pulmonary artery, RCA right coronary artery, TV septal leaflet of tricuspid valve
Fig. 3.4
Relationship between the ascending aorta and the anterior wall of the right atrium. Retracting the aortic root through the recessus between the aorta and the SVC, the operator can see that the anterior wall of the RA is very close to the right coronary cusp and that the posterior half portion of the aortic root has been surrounded by the RA and the LA. The recessus between the aorta and SVC communicates with the transverse sinus of the pericardium cavity normally. This is also the space where the aortic blocking forceps are placed during cardiac surgery. RCA right coronary artery, RV right ventricle, SVC superior vena cava
Fig. 3.5
The relationship between the atrial septum and the septal leaflet of the tricuspid valve. The atrioventricular node (green mark) is located in front of the septal leaflet of the TV and in the posteroinferior portion of the membranous ventricular septum
Fig. 3.6
Interatrial groove. The interatrial groove (the red dash line) is seen from the position of the operator. It is located between the RA and the right pulmonary vein. After loose connective tissues in the groove have been stripped, the LA turns out. The dash line also indicates an important surgical approach to the LA, such as for operations on the MV. MV mitral valve, RPA right pulmonary artery, RPV right pulmonary vein
3.1.2 Morphological Characteristics
The morphology of RA differs from that of the LA by having the following characteristics: (1) a short, blunt, and thin-walled RAA, a piece of triangle-shaped tissue that has more muscle bundles than does the LAA and is a common area for intracardiac detection and cannulation; (2) the orifice of the superior and inferior venae cavae; and (3) the orifice of the coronary sinus vein (Figs. 3.7, 3.8, 3.9, and 3.10). According to the embryonic development, the RA can be divided into two portions, the sinus venosus portion, which is the main portion and is located posteriorly, and the body of the RA. The sinus venosus portion receives systemic venous drainage from the superior and inferior venae cavae and coronary venous drainage from the coronary sinus. The body of the RA is located anteriorly and contains the RAA and the lateral free wall. A muscle bundle called crista terminalis, which has an internodal bundle passing through it, is located between these two portions (Figs. 3.11 and 3.12).
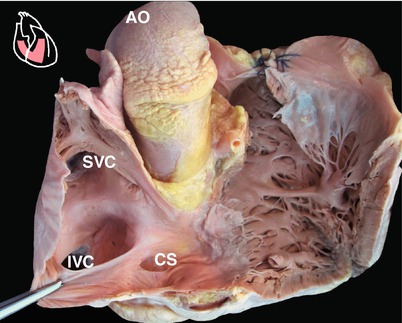
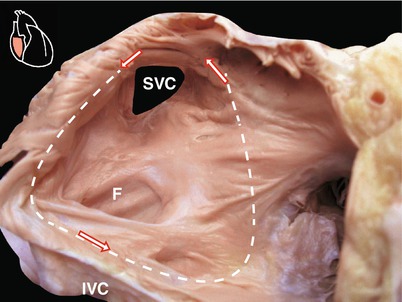
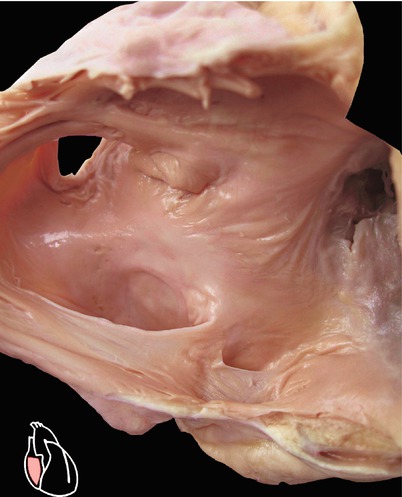




Fig. 3.7
Morphological characteristics of the RA. In contrast to the LAA, the RAA is blunt and large-based. The confirmatory morphological features of the RA are the orifices of the vena cava and the coronary sinus. The smooth wall in front of the vena cava is the sinus venosus portion of the RA, in which the orifices of the vena cava and the coronary sinus are located. This photo shows the structures of the RA and the AV after the anterior wall was resected. CS coronary sinus, IVC inferior vena cava, SVC superior vena cava
Fig. 3.8
Conducting pathway of an atrial flutter. The circular conducting pathway is shown after the anterior wall of the RA has been removed. The wave passes downward along the crista terminalis; follows a course that runs inferior to the coronary sinus and IVC orifice, in front of the FO; and returns to the crista terminalis (Wilcox BR, Cook AC. Surgical Anatomy of the Heart, 3 edition. Cambridge University Press; Cambridge, UK; 2004)
Fig. 3.9
Orifice of the coronary sinus. Located anteroinferior to the orifice of the IVC, the orifice of the coronary sinus is considered to be the posterior margin of the triangle of Koch. This photo shows the relationship of the orifices of the vena cava and the coronary sinus, the FO, and the septal leaflet of TV. This area is very important for atrial septum puncture and surgical procedures in the RA
< div class='tao-gold-member'>
Only gold members can continue reading. Log In or Register to continue
Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
