(1)
Department of General Surgery, Fuwai Hospital, Beijing, China
24.1 General Considerations
24.1.1 Definition
The definition of double-outlet right ventricle (DORV) remains controversial. The consensus is that it is a type of ventriculoarterial connection in which both great vessels arise either or predominantly from the RV. Strictly speaking, the standard is either a semilunar valve that was separated by the cone muscle but is not a fibrous connection or some cone muscle exists between the two semilunar valves if the AV arises more than 90 % from the RV.
24.1.2 Embryological Basis
DORV is a kind of congenital truncal defect characterized by its abnormal absorption and rotation. It could be understood as a transition between the TOF and the TGA.
The two great arteries all arise from the RV in the embryonic stage. With the formation of left and right ventricles and the rotation and absorption of the cone, the PV connects to the RV and the AV connects to the LV. Otherwise, the two arteries would stay at the primary status and develop into a DORV. The cone structure that remains under the two arteries in most of the patients is called the bilateral cone. The two semilunar valves are located side by side, the AV on the right and PV on the left.
24.1.3 Categorization
DORV is always classified according to the following characteristics:
1.
Location of the VSD
2.
With/without pulmonary stenosis
3.
With/without pulmonary hypertension
4.
Associated anomalies
24.1.4 Surgical Application
The LV can connect only with the artery through the VSD because there is no normal outflow tract. As far as the surgical treatment is concerned, the fibrous connection between the semilunar valve and the atrioventricular valve is beneficial to confirm the anomaly. The surgical technique depends on the size of the VSD and the development of pulmonary artery.
Palliative Operation: The pulmonary artery banding can be used in patients with DORV and pulmonary hypertension. A systemic-to-pulmonary artery shunt can be used for patients with pulmonary stenosis.
Radical Operation:
1.
Subaortic VSD with adequate distance between the TV and the PV is treated by simple intraventricular baffling that directs LV blood through the VSD to the aorta.
2.
Subpulmonary VSD without pulmonary stenosis is treated with an arterial switch procedure and a simple VSD closure.
3.
Blood flow in doubly committed VSDs usually is baffled using a more complex patch from the LV to the aorta.
4.
Noncommitted VSD may be treated by baffling of the blood through the VSD to the aorta associated with a myocardial flap reinsertion of the straddling TV or by a Fontan type of procedure.
24.2 Specimen Demonstrations
24.2.1 DORV, AVSD, L-Malposition
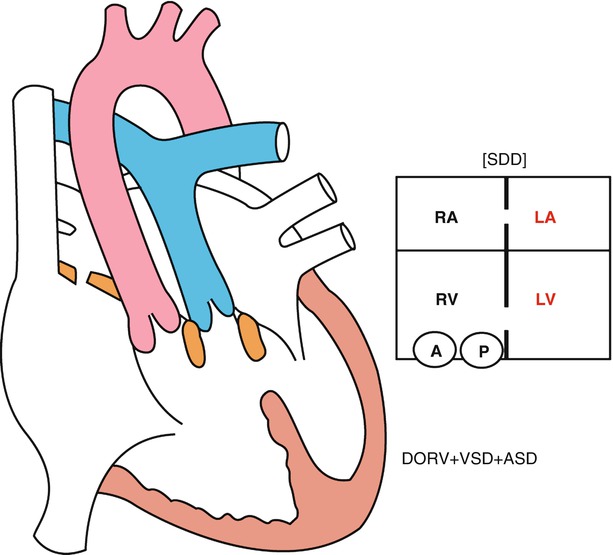
Fig. 24.1
Schematic diagram of common types of DORV. RA right atrium, RV right ventricle, LA left atrium, LV left ventricle, VSD ventricular septal defect, ASD atrial septal defect
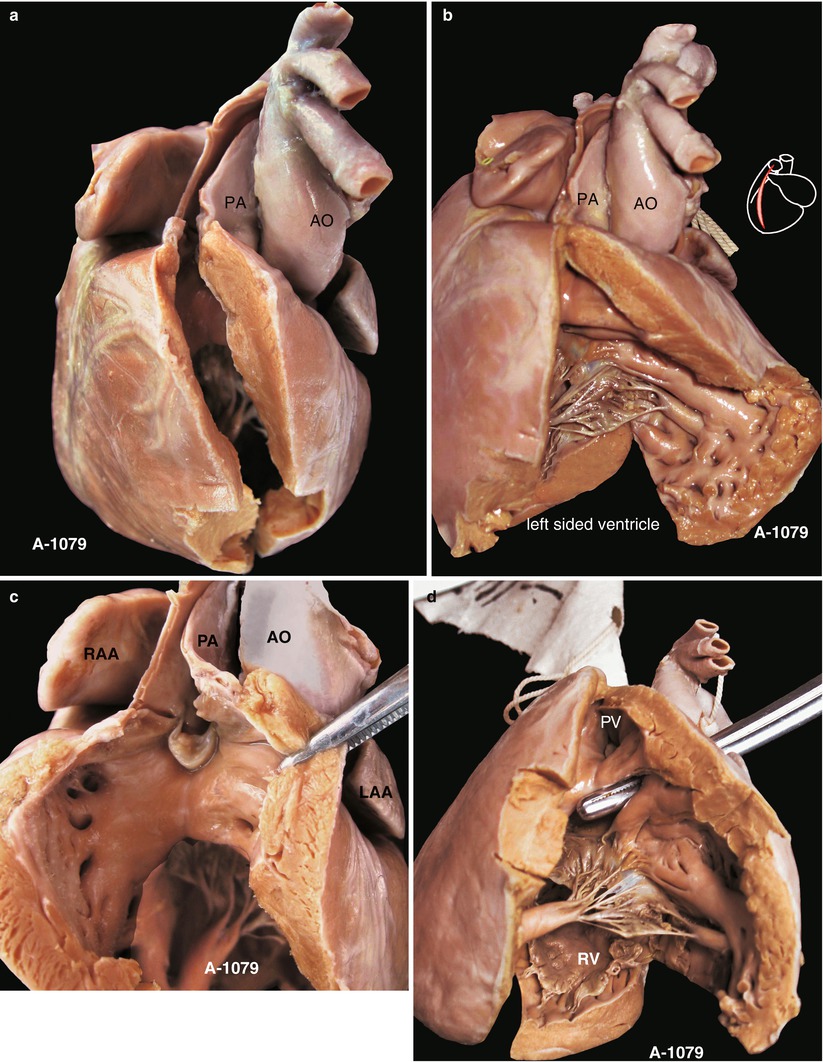
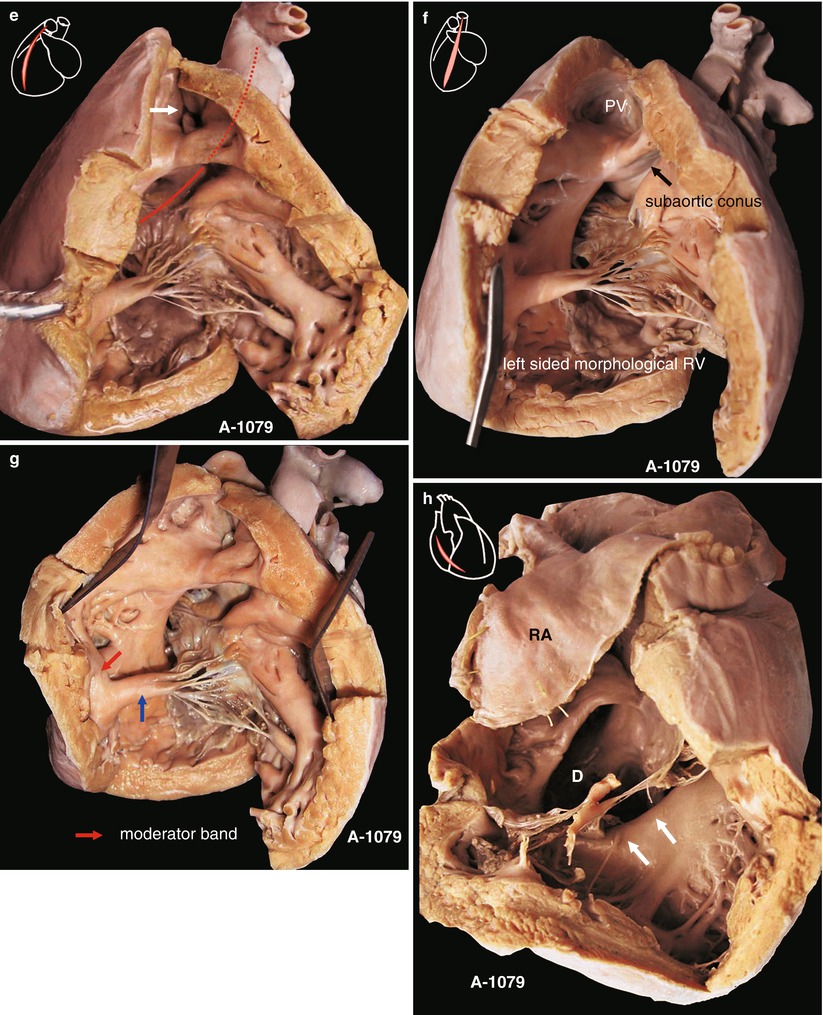
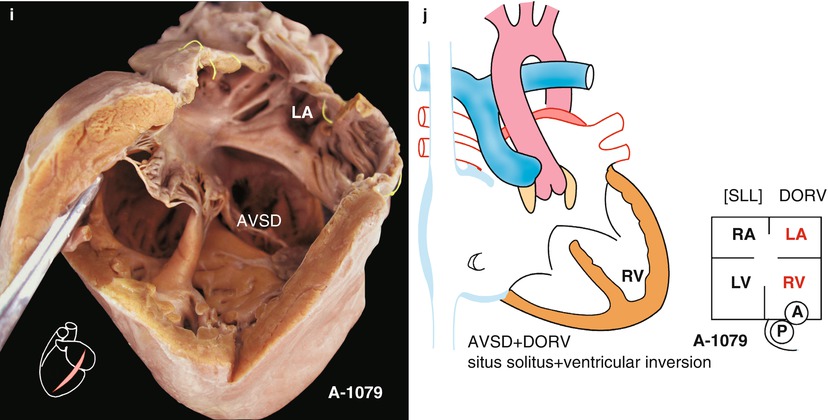
Fig. 24.2
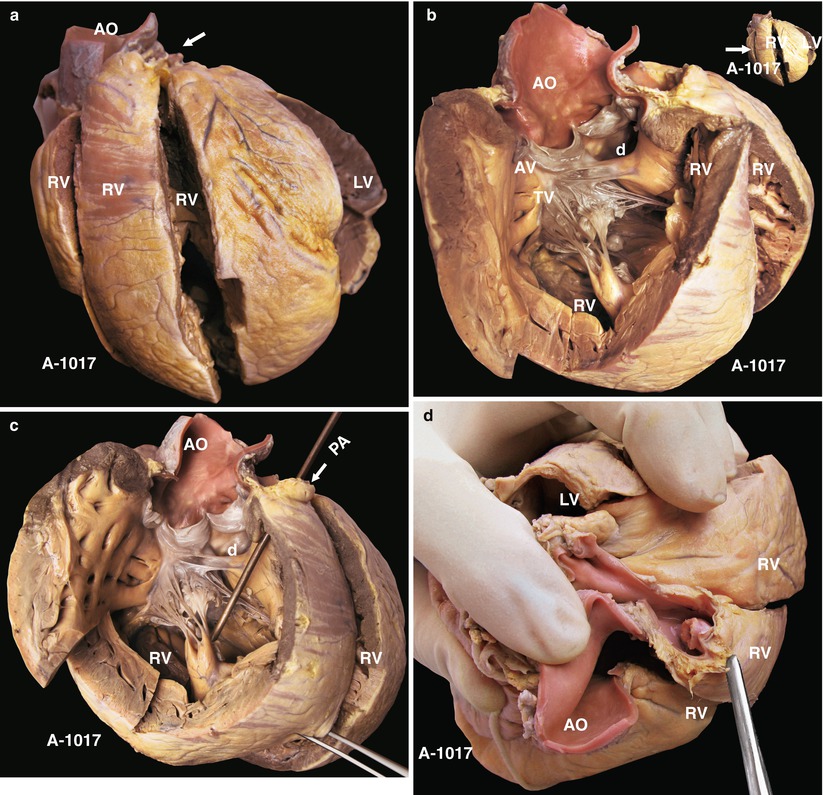
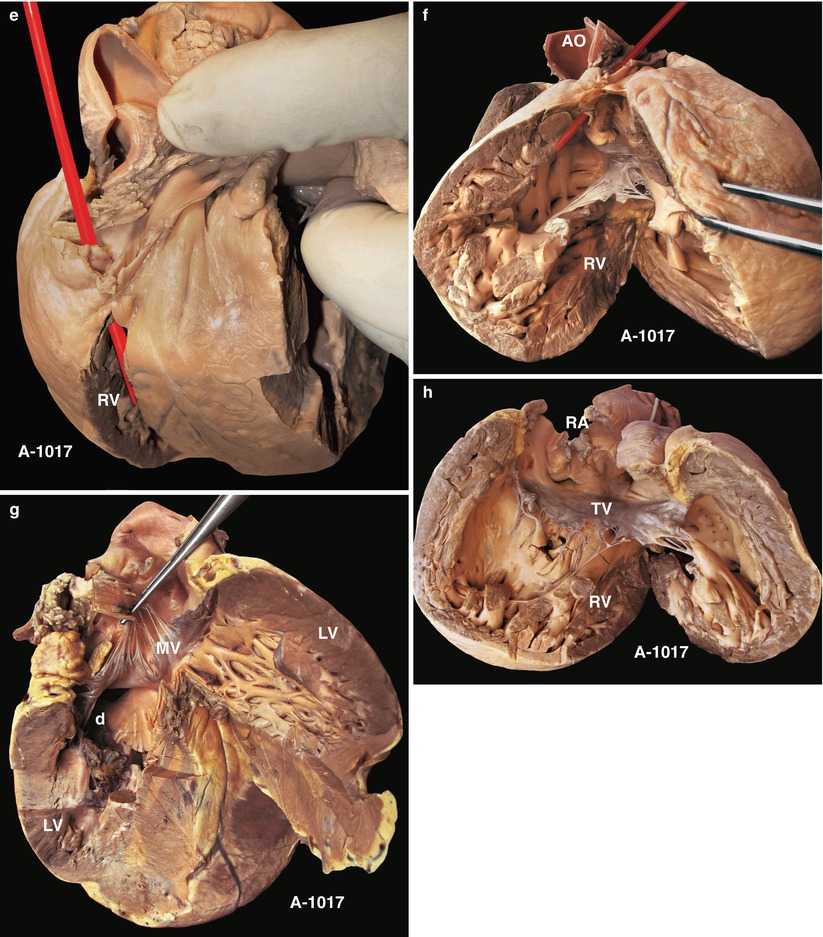
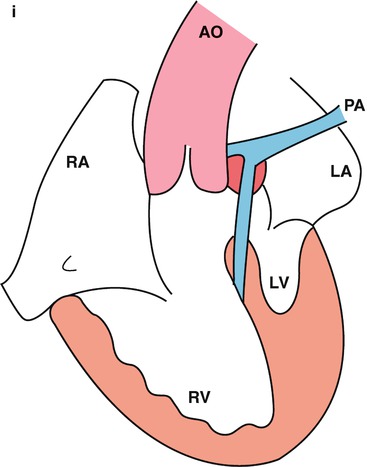
(a) Specimen NO. 1079. DORV with AVSD and L-malposition. Morphological RV is on the left. (b) Specimen NO. 1079. Exposure of the left ventricle to demonstrate the outflow tract and leaflets. The PV is located in the upper right of the AV. (c) Specimen NO. 1079. Demonstration of the pulmonary valve, the thick cone muscle under the valve, and the morphological right ventricle. (d) Specimen NO. 1079. The bougie passing from the aortic valve to the ventricle, and the two muscle bundles under the valve. These characteristics confirmed that the aortic and pulmonary valves arise from the same ventricle. (e) Specimen NO. 1079. Outflow tract of morphological right ventricle. The red line indicates the blood flow in the aorta; the arrow indicates the pulmonary valve. (f) Specimen NO. 1079. Structure of the morphological right ventricle. (g) Specimen NO. 1079. The red arrow indicates the moderator band; the blue arrow indicates the APM. (h) Specimen NO. 1079. Cut of the right atrium and ventricle. An undeveloped right atrioventricular valve forms a common atrioventricular valve with the left one. (i) Specimen NO. 1079. Left-side view of the atrioventricular tract. (j) Schematic diagram of specimen 1079, it’s a heart of complete atrioventricular septal defect. It’s situs sulitus and L-loop. Atrium at right side is right atrium because of it’s connection to vena cava. Atrium at left side is left atrium because of it’s connection to pulmonary vein. PA pulmonary artery, AO ascending aorta, RAA right atrium auricle, LAA left atrium auricle, PV pulmonary valve, RV right ventricle, LA left atrium, AVSD atrioventricular septal defect, RA right atrium, LV left ventricle, D ventricular septal defect
24.2.2 A Typical DORV Is Seen
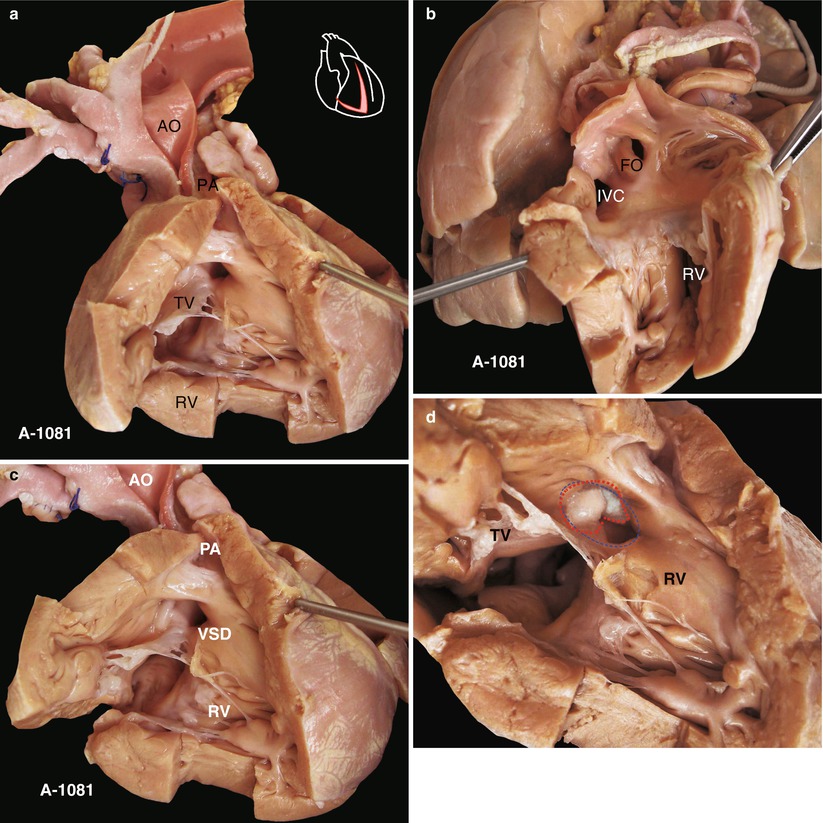
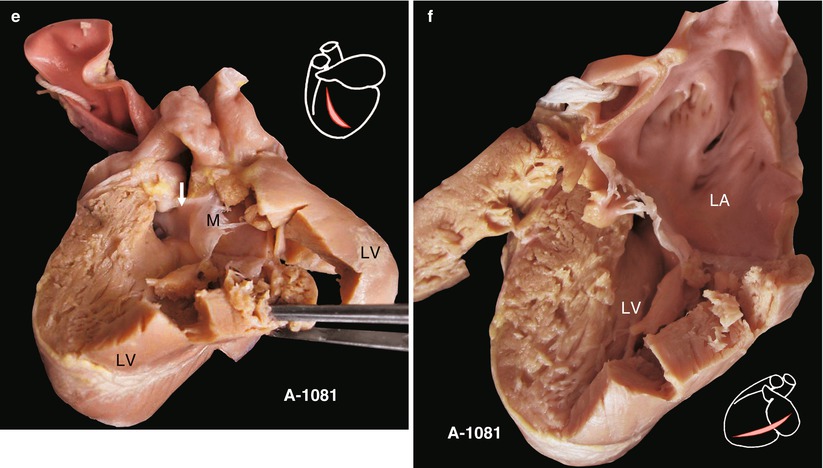
Fig. 24.3
(a) Specimen NO. 1081. Specimen of DORV. (b) Specimen NO. 1081. Exposure of the right atrium and ventricle to demonstrate its inflow tract. (c) Specimen NO. 1081. Demonstration of the outflow tract of the right ventricle. (d) Specimen NO. 1081. Exposure of the VSD from the outflow tract of the right ventricle. The AV overlies the VSD. (e) Specimen NO. 1081. Left ventricle cut to demonstrate its outflow tract. (f) Specimen NO. 1081. Left atrium and ventricle cut to demonstrate the left atrium, the mitral valve, and the inflow tract. AO ascending aorta, PA pulmonary artery, TV tricuspid valve, RV right ventricle, FO fossa ovalis, IVC inferior vena cava, VSD ventricular septal defect, M mitral valve, LV left ventricle, LA left atrium
24.2.3 DORV, Dextrocardia, and Exterior Channel Surgery are Shown
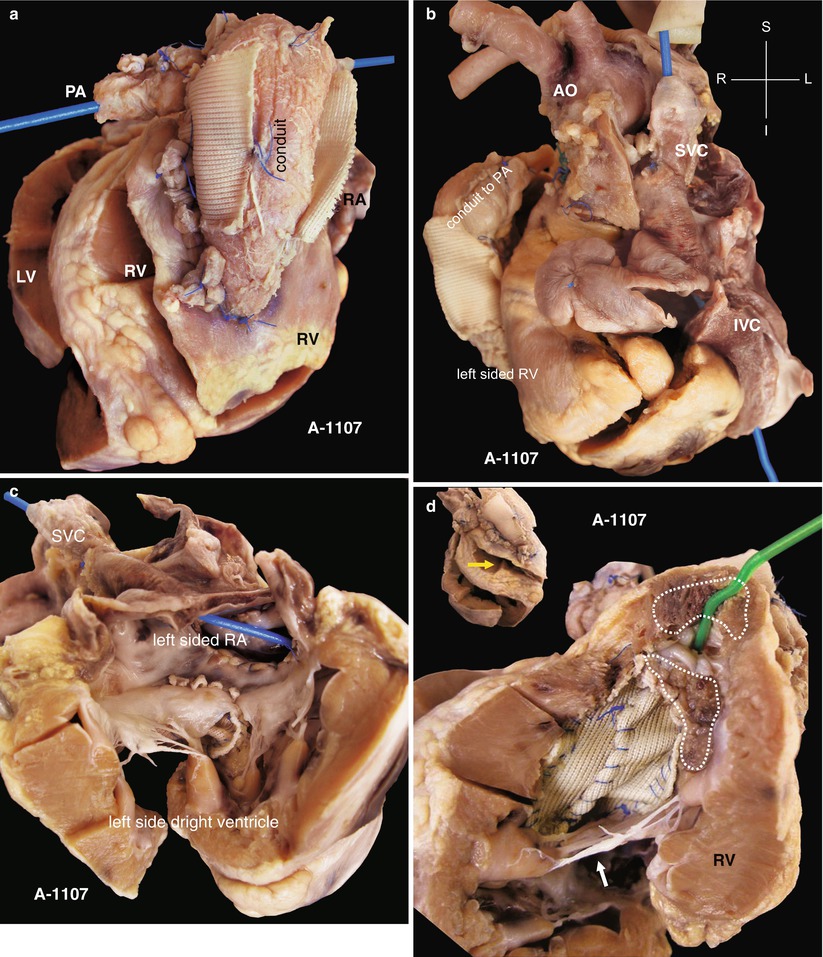
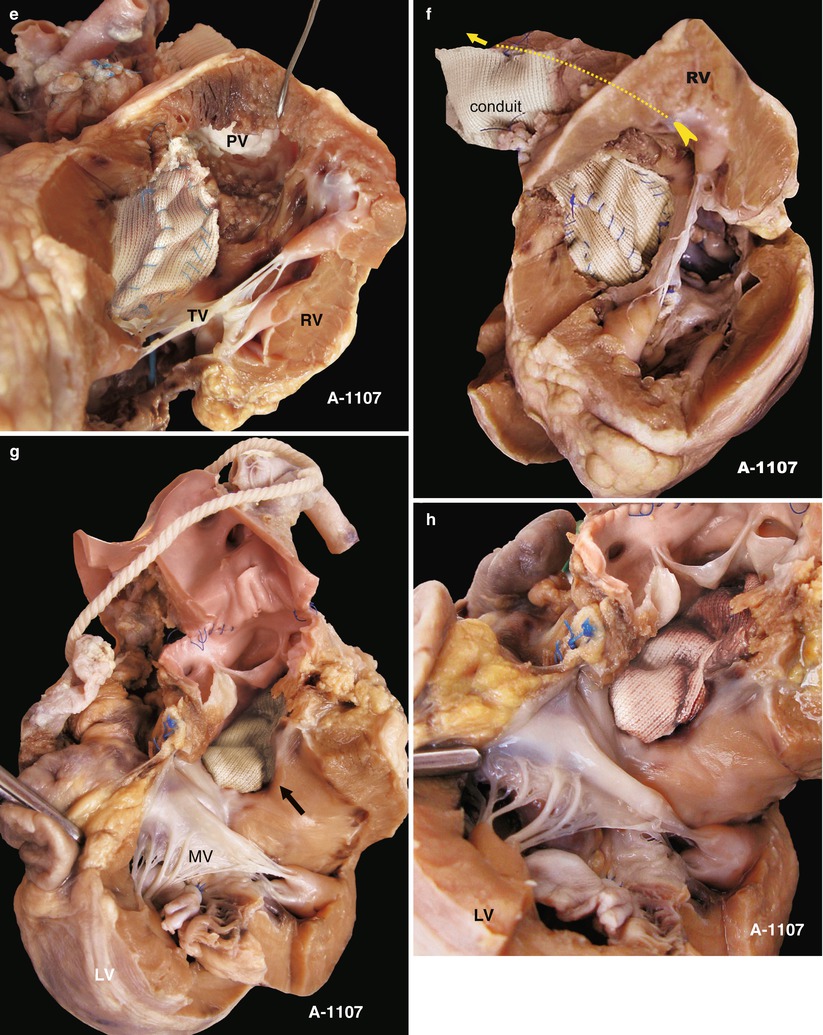
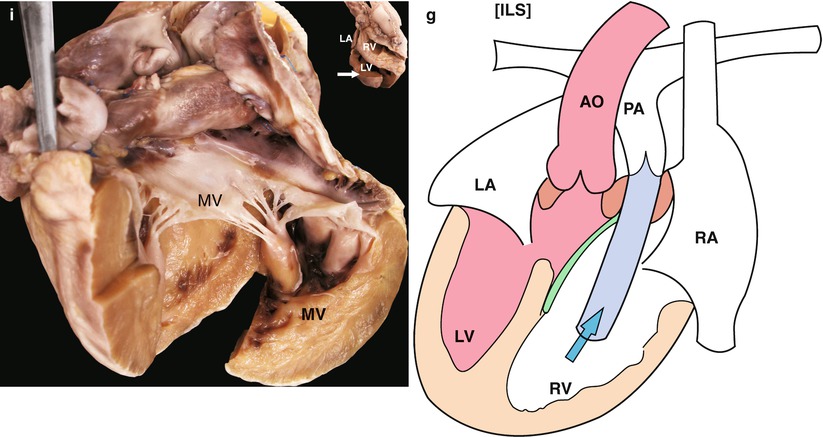
Fig. 24.4
(a) Specimen NO. 1107. DORV and dextrocardia, pulmonary stenosis. RV connects with the pulmonary artery with graft. (b) Specimen NO. 1107. Left anterior oblique view. RA and RV are on the left; bougie is in the vena cava. (c) Specimen NO. 1107. Left-side view. RA and RV are on the left; the VSD patch is in the TV. (d) Specimen NO. 1107. Opened outflow tract of the right ventricle. The aorta and PV arise from the RV. (e) Specimen NO. 1107. Clearer demonstration of the structure under the pulmonary valve. (f) Specimen NO. 1107. Dotted line indicates the connection of RV and the exterior channel. (g) Specimen NO. 1107. The MV is away from the AV, there is no fibrous connection, and the AV arises from opposite RV. The arrow indicates the VSD patch, which forms a part of LVOT. (h) Specimen NO. 1107. The same figure with 24-4 g with closer observation. (i) Specimen NO. 1107. Exposure of the left atrium and ventricle on the right. (j) Specimen NO. 1107. Schematic diagram of specimen 1107. PA pulmonary artery, PV pulmonary valve, RV right ventricle, LA left atrium, AO ascending aorta, RA right atrium, LV left ventricle, TV tricuspid valve, IVC inferior vena cava, SVC superior vena cava, MV mitral valve, PV pulmonary vein
24.2.4 DORV, Hypoplasia of Pulmonary Artery
Only gold members can continue reading. Log In or Register to continue
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


