(1)
Department of General surgery, Fuwai Hospital, Beijing, China
8.1 General Considerations
8.1.1 Wall of the Left Ventricle
The ventricular wall is separated from the LA by the atrioventricular groove, from which the coronary sinus and the LCx extend. The left ventricular anterior wall is demarcated from the RV by the interventricular sulcus, an important marker of the LV and in which is found the LAD (Fig. 8.1).
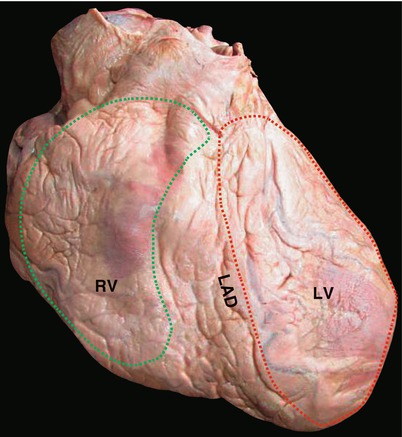
Fig. 8.1
Left anterior oblique view of heart showing the left ventricular lateral wall. The portion behind the LAD is the lateral wall of the LV (area encircled by red dotted line). The green dotted line indicates the RV. LAD left anterior descending artery, LV left ventricle, RV right ventricle
8.1.1.1 Characteristics
The left ventricular wall is formed by the twisted myocardial bands that anchor to the cardiac fibrous skeleton at the upper end, forming the left ventricular orifices, namely, the left atrioventricular valve and the AV, that constitute the apex. The myocardial bands consist of the superficial, middle, and deep layers of spiral muscles, which twist and form the entire left ventricular wall (Fig. 8.2). Some of the myocardial bands take part in forming the RV and the interventricular septum, which is evidently thicker in the left ventricular wall than in the right counterpart (Fig. 8.3).
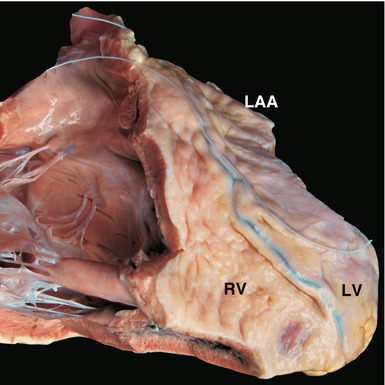
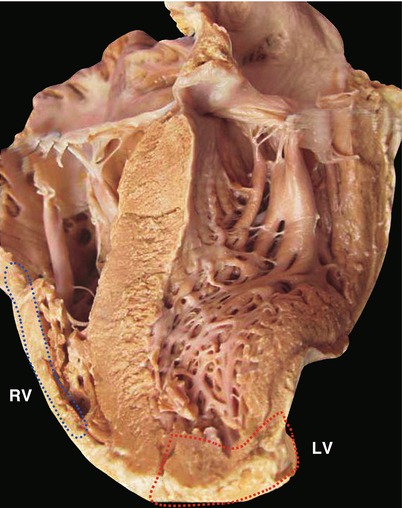
Fig. 8.2
Comparison of the morphologies of the left and right ventricles. The front wall of the RV is removed. Viewing the front of the heart, the interventricular septum convexes to the right, rendering the LV a cone-shaped cavity, while the RV attaches to the right of the LV. LAA left atrial appendage, LV left ventricle, RV right ventricle
Fig. 8.3
Comparison of left and right ventricular walls. The coronal section demonstrates the walls of the left and right ventricles. The area enclosed in the red dotted line indicates the left ventricular wall. The blue dotted line encloses the right ventricular wall. The LV works in systemic circulation, so its wall is apparently thicker than the right ventricular wall
The left ventricular wall is mortar shaped and formed by thick and strong muscles, in contrast to the thin right ventricular wall (Figs. 8.4, 8.5, and 8.6). This difference of structures between two ventricles reflects their physiological functions: the LV bears the resistance of systemic circulation.
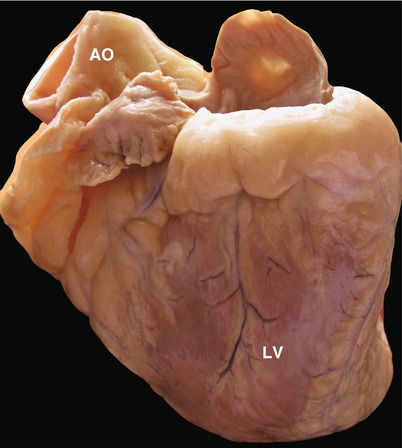
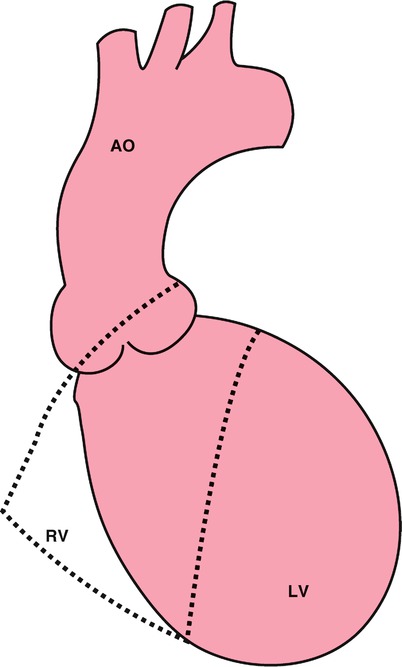
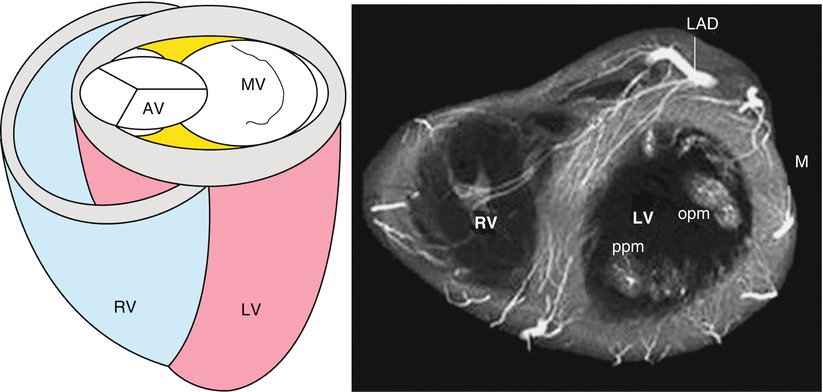
Fig. 8.4
Mortar-shaped left ventricle with coronary vessels on the surface. The wall of the LA is removed, leaving the LAA and the interatrial septum. LA left atrium, LAA left atrial appendage
Fig. 8.5
Projection of the front view of the left ventricle. The shapes and relationship of the left and right ventricles are demonstrated. The blue dotted line depicts the RV closely adjoining the LV
Fig. 8.6
Illustration of the transaction of the ventricles. The LV is a mortar-shaped muscular pump. The upper orifices include the inlet orifice (the MV) and outlet orifice (the AV). AV aortic valve, MV mitral valve, RV right ventricle
8.1.1.2 Wall Portions
The left ventricular wall is divided into three portions:
(a)
Interventricular septum
This portion is composed of thick and strong myocardial tissue. The interventricular septum separates the two ventricles; it concaves in the left side and convexes in the right side. The upper end of the septum connects to the right coronary sinus of the aorta. The muscular part of the septum is connected with the central fibrous body at the membranous part, which is small. The conduction bundle passes underneath it (Figs. 8.7 and 8.8).
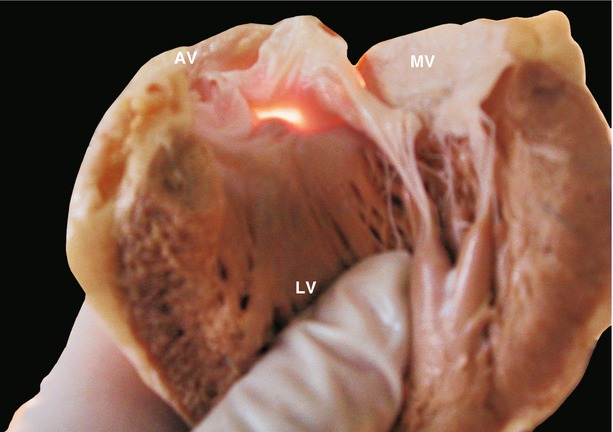
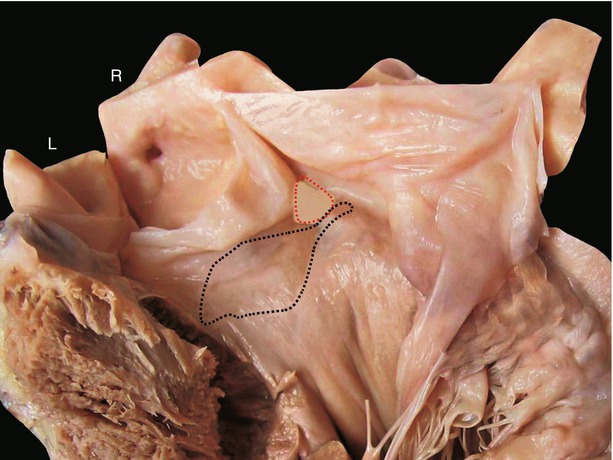
Fig. 8.7
Membranous interventricular septum. The left ventricular lateral wall is removed. The membranous septum (the semitransparent area) is observed from the left ventricular cavity
Fig. 8.8
Membranous interventricular septum and left bundle branch. The interventricular septum is displayed from the left ventricular cavity. The membranous septum (red dotted line) lies beneath the commissure between the right and noncoronary cuspids. The septum beneath the left and right aortic cuspids is incised. The left bundle branch (blue dotted line) passes subendocardially on the left side of the interventricular septum beneath the membranous septum. L left coronary cuspid, R right coronary cuspid
(b)
Diaphragmatic side of the left ventricular wall
This portion connects with the diaphragm and is hard to expose.
(c)
Free ventricular wall in the left anterior of the free ventricular wall in the left anterior of the LV, separated from the RV by the interventricular sulcus; within it passes the LAD.
The LCx extends into the atrioventricular groove. The avascular area behind the interventricular sulcus is the preferable site for performing a ventriculoplasty.
8.1.2 Cavity of the Left Ventricle
The left ventricular cavity can be divided into the sinus portion, the trabeculated portion, and the outlet portion or tract.
8.1.2.1 Sinus Portion
The sinus portion is the inlet tract of the LV and has a smooth inner wall.
8.1.2.2 Trabeculated Portion
The trabeculated portion is at the apex and has trabeculae of different sizes. Two groups of trabeculae of larger sizes form the papillary muscles of the MV.
8.1.2.3 Outlet Tract
The left ventricular outlet tract (LVOT) is encircled by a muscular interventricular septum and fibrous continuity of the mitral-aortic valve. The right coronary sinus of the aorta is tightly adhered to the interventricular septum (Figs. 8.9 and 8.10). The septum is smooth with a fan-shaped left branch of the conduction bundle extending in the superficial layer (Fig. 8.8). There is neither complete infundibular muscle nor muscle bands as in the supraventricular crest of the RV. The continuity of the anterior leaflet of the MV and of the leaflets of the AV appears to be like a screen, separating the inlet portion from the LVOT and forming the membranous portion of the left ventricular outlet tract (Fig. 8.9). The interventricular septum forms the muscular portion of the LVOT. The existence of the fibrous continuity of the anterior leaflet of the MV and the leaflets of the AV is one of the important identifications of congenital cardiac deformities.
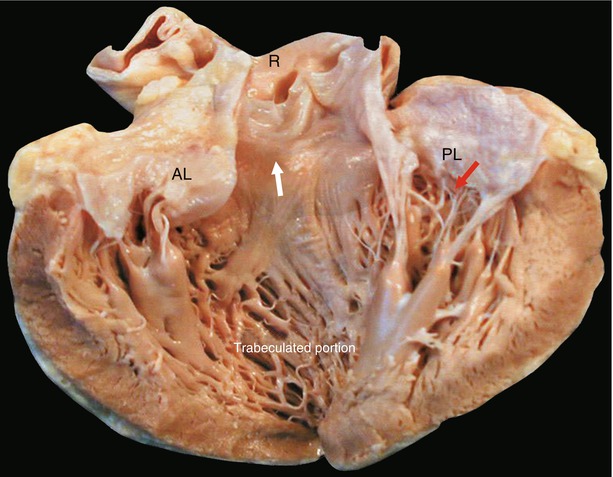
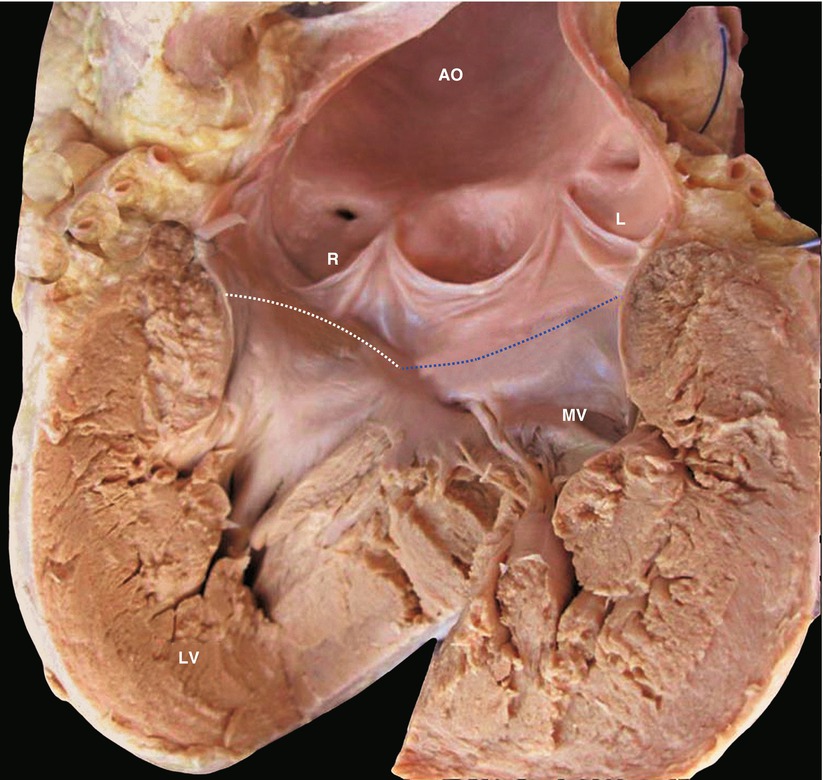




Fig. 8.9
Inlet and outlet tracts of the left ventricle. The specimen is dissected along the LVOT to display the overall view of the LV. The red arrow indicates the inlet tract (i.e., the MV). The white arrow indicates the outlet tract. The anterior wall of the outlet tract is the interventricular septum, whereas the posterior wall is the anterior mitral leaflet. AL anterior mitral leaflet, LV left ventricle, LVOT left ventricular outlet tract, PL posterior mitral leaflet, R right coronary cuspid. Surgical implications: In hypertrophic obstruction of the LVOT, one of the surgical procedures is to excise some of the interventricular septal muscles at the site indicated by the white arrow, where, by accident, the interventricular septum could be perforated to enter the RV and the AV and the papillary muscles of the MV would be injured. Another surgical procedure is MV replacement, thus eliminating the anterior movement of the anterior mitral leaflet in systole, which exacerbates the obstruction of the LVOT
Fig. 8.10
Upper border of the left ventricular outlet tract. The LVOT is dissected from the apex to the aorta. The upper border of the outlet tract is composed of the attaching margin of the aortic cuspids on the interventricular septum (white dotted line) and the joint line of the aortic-mitral fibrous continuity (blue dotted line). L left coronary cuspid, MV anterior mitral leaflet, R right coronary cuspid
< div class='tao-gold-member'>
Only gold members can continue reading. Log In or Register to continue
Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
