(1)
Department of General surgery, Fuwai Hospital, Beijing, China
7.1 Structure and Characteristics of the Left Atrium
The left atrium (LA) lies behind the ascending aorta and is superior to the LV (Figs. 7.1, 7.2, and 7.3). The LA is demarcated from the LV by the atrioventricular groove, within which lie the LCx and the coronary sinus.
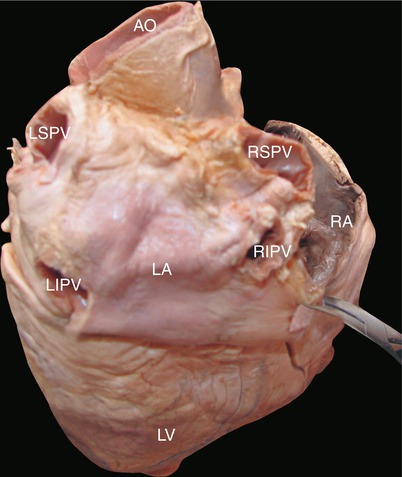
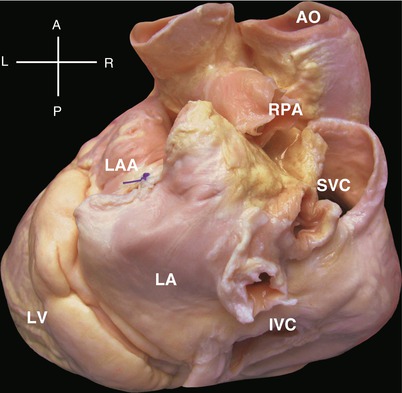
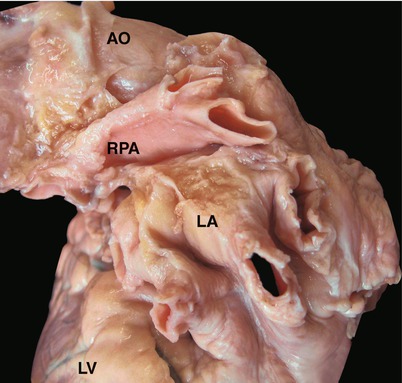
Fig. 7.1
Position of the LA. Figure shows anatomical view of the dorsal part of the heart. The LA lies behind the aorta and above the ventricles. The RA is on the right side of the LA. The left atrioventricular groove is between the LA and the LV. Four orifices of the pulmonary veins lie in the posterior wall of the LA. AO aorta, LA left atrium, LIPV orifice of left inferior pulmonary vein, LSPV orifice of left superior pulmonary vein, LV left ventricle, RA right atrium, RIPV orifice of right inferior pulmonary vein, RSPV orifice of right superior pulmonary vein
Fig. 7.2
Neighboring of the LA. Overview of the heart from the left posterior side shows neighboring relations of the LA and superior vena cava (SVC), inferior vena cava (IVC), right pulmonary vein (RPV), left atrial appendage (LAA), left ventricle (LV), right pulmonary artery (RPA)
Fig. 7.3
Right pulmonary vein above the LA. The right pulmonary vein (RPA) extends across the roof of the LA. AO ascending aorta, LA left atrium, LV left ventricle
7.1.1 Structure
Similar to the RA, the LA consists of trabecular and sinus portions (Fig. 7.4). The trabeculated part, confined within the LA appendage, is developed from preliminary LA of the embryonic heart (Fig. 7.5). The LAA is a triangular protrusion with several exterior incisurae and interior cavernous trabeculae (Fig. 7.6). The sinus portion is developed from the dorsal bulge of the embryonic LA, which becomes the common pulmonary venous trunk, joining the pulmonary veins and eventually becoming enlarged (Fig. 7.4). The LA has a smooth interior, with four pulmonary veins entering dorsally. Posteroinferiorly, the LA adjoins the posterior annulus of the MV and coronary sinus, where it is called the vestibule of the left artery (Fig. 7.7). In an abnormally enlarged LA, the posteroinferiorly enlarged vestibule results in the displacement of the MV annulus. The LA volume reduction surgery is performed in the left atrial vestibule.
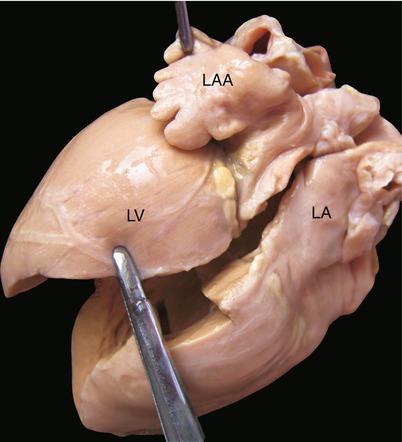
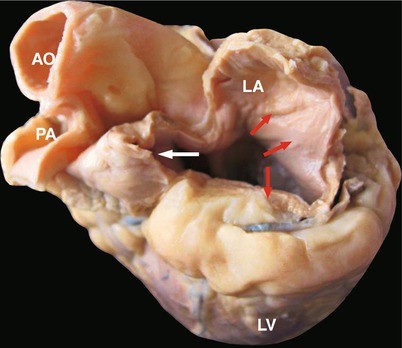
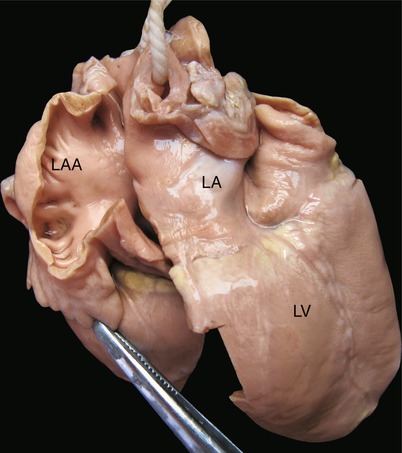
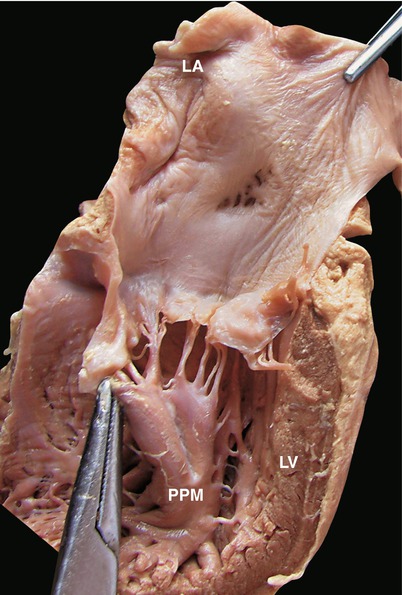
Fig. 7.4
Incisurae on the neck of the left atrial appendage. The anatomical view from the left side displays the LA and LAA. In contrast to the RAA, the neck of the LAA is slender and narrow with exterior incisurae and interior trabeculae. The wall of the LAA is thin and fragile. Cautions should be taken to avoid incision avulsion during cannulation and finger exploration, which, in severe cases, can result in massive bleeding and injury to the left circumflex artery. LV left ventricle
Fig. 7.5
Compartments of the left atrial cavity. The specimen is viewed from the left side. The lateral wall of the LA is removed. The white arrow indicates the cavity of the LAA, which is trabecular. The red arrow indicates the main part of the LA and its smooth inner wall, where the pulmonary veins emerge in the embryonic period. AO aorta, LA left atrium, LAA left atrial appendage, LV left ventricle, PA pulmonary artery
Fig. 7.6
Trabeculae of the left atrial appendage. The LAA is incised, revealing the trabeculated portion. LV left ventricle, LA left atrium
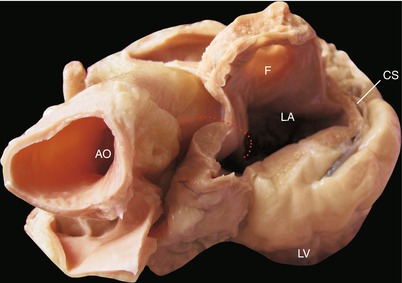
Fig. 7.7
Inner wall of the left atrium. The sagittal section viewed from the left side shows the reticular fold on the center of the left side of the interatrial septum, corresponding to the FO on the right atrial side of the septum. The posterior leaflet and the PPM of the MV are also displayed. FO fossa ovalis, PPM posterior papillary muscle, LV left ventricle, LA left atrium
The posterior wall of the LA joins the entries of the four pulmonary veins (Fig. 7.1); being deep and immobile, it is hard to access during surgery. The inner wall of the LA is smooth. The LA closely adjoins the esophagus dorsally. When enlarged, the LA pushes the esophagus rightward and backward. An oblique ligament located lateral to the posterior wall of the LA and extending inferiorly and rightward is the relic of regressed embryonic oblique veins. If incompletely regressed, it remains the persistent left superior vein, which connects the cephalobrachial vein superiorly and the coronary sinus inferiorly. One should be alert to its possible presence when inspecting the enlarged coronary sinus orifice. The LAA is well exposed through the left lateral thoracotomy, which is the ideal route for LA exploration.
The roof of the LA is located beneath the aortic arch and the right pulmonary artery (Fig. 7.6). Dorsally, the LA neighbors the tracheal bifurcation, which can be lifted by an enlarged LA.
The interatrial septum lies between the left and right atria. The semilunar fold on the left side of the interatrial septum, which is the relic of the primary interatrial septum, is an important marker for identifying the LA. The anterior wall of the LA closely neighbors the ascending aorta, where it is separated from the left and part of the noncoronary sinus. The anterior wall of the LA continues downward to the base of the anterior leaflet of the MV, where, together with the aortic annulus, it forms the converging part and is the site of incising the LA and the anterior leaflet of the MV during an aortic annular enlargement procedure (Figs. 7.8 and 7.9).
 < div class='tao-gold-member'>
< div class='tao-gold-member'>




Only gold members can continue reading. Log In or Register to continue
Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
